
SEPTEMBER 2022 Issue Brief 1
Trends in Prescription Drug Spending, 2016-2021
KEY FINDINGS
• In 2021, the U.S. health care system spent $603 billion on prescription drugs, before accounting for rebates, of
which $421 billion was on retail drugs.
• Spending growth on drugs was largely due to growth in spending per prescription, and to a lesser extent by
increased utilization (i.e., more prescriptions).
• Expenditure growth was larger for non-retail drug expenditures (25%) than for retail expenditures (13%).
• Between 2016 and 2021, the location where people received their drugs changed. Americans increasingly
received their drugs from mail order pharmacies (35% increase), clinics (45% increase), and home health care
(95% increase). During the same time period, there were decreases in drugs received through independent
pharmacies (5% decrease), long term care facilities (17% decrease), and federal facilities (9% decrease).
• Drug spending is heavily driven by a relatively small number of high-cost products. The cost of specialty drugs
has continued to grow, totaling $301 billion in 2021, an increase of 43% since 2016. Specialty drugs
represented 50% of total drug spending in 2021. While the majority (80%) of prescriptions that Americans fill
are for generic drugs, brand name drugs accounted for 80% of prescription drug spending in both retail and
non-retail settings, with little change over time. The top 10% of drugs by price make up fewer than 1% of all
prescriptions, but account for 15% of retail spending and 20%-25% of non-retail spending.
• Prescription drug spending trends have been less affected by the COVID-19 pandemic than health care
services.
• Several provisions in the Inflation Reduction Act address drug pricing, including allowing the Secretary of HHS
to negotiate prices in Medicare Parts B and D for selected medications and introducing Medicare rebates for
drug prices that rise faster than inflation. These provisions may impact future drug spending trends.
Introduction
High prescription drug costs are a leading concern among Americans.
1
Americans pay higher prices for
prescription drugs than any other country in the world, with prescription drug prices in the U.S. more than 2.5
times as high as those in other similar high-income nations.
2
To support the Administration’s efforts to make
drug prices and spending more transparent, the goal of this brief is to present the drivers of total spending on
prescription drugs between 2016 and 2021. The analyses are disaggregated for retail drugs and non-retail drugs.
We also examine spending specifically on brand name drugs, specialty drugs, and the top 10% of drugs by price.
By examining trends over time, we capture changes in prescription drug spending during the COVID-19
pandemic.
1
Bush, L and Sommers, B.D. (2022). Improving Prescription Drug Affordability Through Regulatory Action. JAMA Health Forum 3(8).
2
Mulcahy, A.W., Whaley, C., Tebeka, M.G., Schwam, D., Edenfield, N., and Becerra-Ornelas, A.U. “International Prescription Drug Price
Comparisons: Current Empirical Estimates and Comparisons with Previous Studies,” RAND Research Report RR-2956-ASPEC, 2021.
Available at: https://aspe.hhs.gov/sites/default/files/documents/ca08ebf0d93dbc0faf270f35bbecf28b/international-prescription-drug-
price-comparisons.pdf.
OFFICE OF
SCIENCE & DATA POLICY
ISSUE BRIEF
SEPTEMBER 2022

SEPTEMBER 2022 Issue Brief 2
Methods
Data
The primary data for this analysis were IQVIA National Sales Perspective (NSP) data from 2016 through 2021.
3
IQVIA data are derived from a panel of wholesalers, distributors, and pharmaceutical manufacturers that
represent 90% of the pharmaceutical market and are projected to be nationally representative.
3
We examined two primary outcomes of interest: prescription drug spending and number of prescriptions.
Prescription drug spending was measured in inflation adjusted dollars.
4
The IQVIA dataset reports gross drug
spending, meaning it does not include rebates.
5
The number of prescriptions was calculated as a measure of the
number of units of a drug a manufacturer sold to a wholesaler or pharmacy. The data are at the drug claim level
and include where an individual received drugs (i.e., retail or non-retail dispensers). Retail drugs were defined as
those that are filled in an outpatient setting, including standalone pharmacies and mail order prescriptions. Non-
retail drugs were defined as those administered in an inpatient setting, including hospitals, clinics, physician
offices, long term care facilities, and home health. Non-retail spending on prescription drugs was one of the
fastest drivers of prescription drug spending; thus, capturing these prescriptions was critical to understanding
current prescription drug spending trends.
The drug attributes of interest included brand name and generic drugs, specialty drugs, and the top 10% of
drugs based on price. The top 10% of drugs by price were defined on an annual basis, meaning the drugs change
for each year of the sample.
6
Results
Total Spending Trends
Table 1 shows the number of prescriptions and drug expenditures from 2016 to 2021. Total inflation-adjusted
expenditures on prescription drugs grew from $520 billion in 2016 to $603 billion in 2021, a 16 percent increase.
This rate of growth was similar to overall national health care spending growth, with prescription drugs
maintaining approximately an 18 percent share of total health care expenditures throughout this time period.
Overall, retail drug expenditures represented roughly 70% of prescription drug spending and non-retail 30%.
We then examined trends broken out by retail and non-retail drugs. There was a 13 percent increase in retail
prescription drug spending over this five-year period, but only a 5.7 percent increase in the number of retail
prescriptions. On average, there was a 7 percent increase in spending per prescription, which suggests that
changes in utilization (i.e., a greater number of prescriptions being filled) were not the primary driver of
increased retail drug spending. For non-retail drugs, we observed a 25 percent increase in expenditures and a 19
percent increase in the number of prescriptions. On average, there was a 5 percent increase in the spending per
prescription, meaning that the primary driver of increased non-retail prescription drug spending was greater
utilization, rather than higher drug prices. The growth in non-retail prescriptions, 19 percent, was 3.4 times
higher than the increase in prescriptions for retail drugs.
3
Source of the data: IQVIA. U.S. National Data. <https://www.iqvia.com/insights/the-iqvia-institute/available-iqvia-data>.
4
The spending data includes an adjustment for inflation, thereby representing a “real” dollar. The data represent the value of a real
dollar as of quarter 1 of 2022. Source: U.S. Bureau of Economic Analysis, Gross Domestic Product: Implicit Price Deflator [GDPDEF],
retrieved from FRED, Federal Reserve Bank of St. Louis; https://fred.stlouisfed.org/series/GDPDEF, August 19, 2022.
5
Retail drugs can be subject to rebates while non-retail drugs do not have rebates. As a result, retail drug spending may be overestimated
relative to non-retail spending and personal health expenditures (the NHEA estimates are net of rebates for retail drug spending).
6
More details about the variable specifications can be found in the appendix.
SEPTEMBER 2022 Issue Brief 3
Table 1. Prescription Drug Expenditures (in Inflation Adjusted Dollars) and Prescriptions, 2016-2021
Retail
Expenditures
Billions, $
Retail
Prescriptions
Millions
Non-Retail
Expenditures
Billions, $
Non-Retail
Prescriptions
Millions
Total
Expenditures
Billions, $
Total
Prescriptions
Millions
2016
374
4,816
146
3,066
520
7,882
2017
369
4,923
151
3,097
519
8,020
2018
377
5,118
163
3,214
540
8,332
2019
389
5,243
173
3,486
562
8,729
2020
406
4,970
176
3,509
582
8,479
2021
421
5,089
182
3,654
603
8,743
% Change
2016-2021
12.5%
5.7%
25.1%
19.2%
16.0%
10.9%
Source: ASPE analysis of IQVIA National Sales Perspective (NSP) Data. All dollar amounts include an adjustment for inflation so they
represent a “real dollar” as of quarter 1 of 2022.
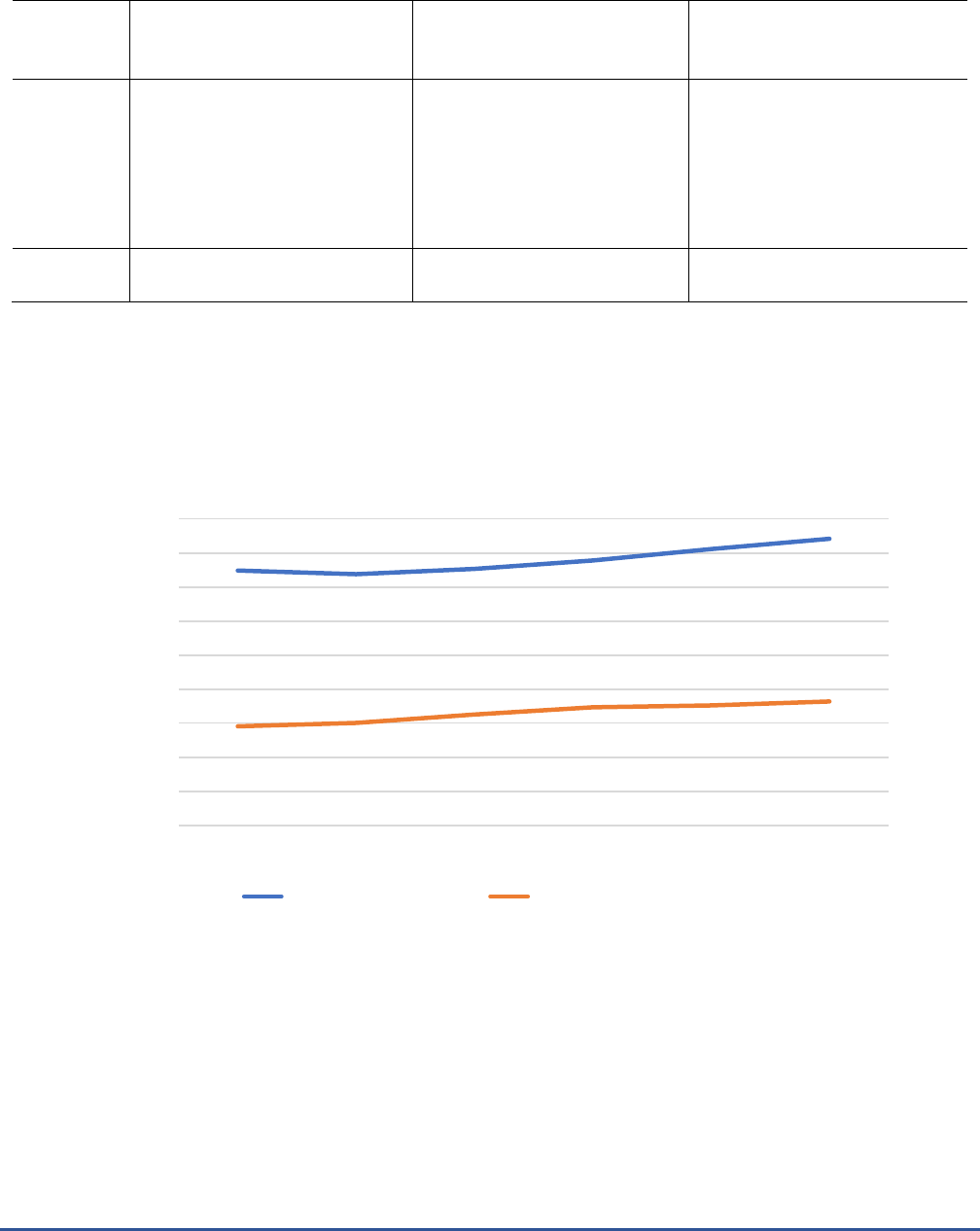
Figure 1 shows the change in retail and non-retail expenditures between 2016 and 2021. Similar to Table 1, we
observe growth in both retail and non-retail drug expenditures, with a slightly faster rate of growth for non-
retail drug spending.
Figure 1. Spending (in Inflation Adjusted Dollars) on Retail and Non-Retail Drugs, 2016-2021
Source: ASPE analysis of IQVIA National Sales Perspective Data. All dollar amounts include an adjustment for inflation so they represent a
“real dollar” as of quarter 1 of 2022.
Location of Sale
Table 2 shows the breakdown of spending over time by location of sale. There were four locations of sale for
retail drug expenditures – chain store pharmacy, mail order pharmacy, independent pharmacy, and food store
pharmacy. Three of the four locations experienced an increase in sales between 2016 and 2021. Expenditures
increased by 4 percent in chain store pharmacies, 35 percent for mail order pharmacies, and 1 percent for food
store pharmacies, but decreased 5 percent for independent pharmacies.
0
50
100
150
200
250
300
350
400
450
2016 2017 2018 2019 2020 2021
Billions of Inflation Adjusted Dollars
Retail Expenditures Non-Retail Expenditures

SEPTEMBER 2022 Issue Brief 4
For non-retail drug spending, there were more potential locations of sale, but the majority of these locations
dispensed small volumes of drugs. Over the full five-year period, the most common location of sale for non-
retail drug expenditures were clinics. Spending in clinics increased from $76 billion in 2016 to $110 billion in
2021, a 45 percent increase. The other location with substantial sales of non-retail drugs were non-federal
hospitals. Non-federal hospitals spent $39 billion on non-retail drugs in 2016 which increased by 4 percent to
$41 billion in 2021. The location with the largest increase in use was home health care, where there was a 95
percent increase from 2016 through 2021. Five locations of sale experienced declines in non-retail drug
expenditures over the time span. These was a 31 percent drop in non-retail drug spending in universities, a 17
percent drop in non-retail expenditures in long term care facilities, a 15 percent drop in “other” non-retail
settings, a 10 percent drop in prison non-retail drug expenditures, and a 9 percent drop in federal facilities.
Table 2. Expenditures (in Inflation Adjusted Dollars) on Drugs Based on Location of Sale, 2016-2021
Location of Sale
2016
2017
2018
2019
2020
2021
% Change
2016-2021
Billions, $
Retail
Chain Store Pharmacy
161
154
156
158
164
167
4
Mail Order Pharmacy
123
128
136
146
158
166
35
Independent Pharmacy
58
57
56
55
54
55
-5
Food Store Pharmacy
32
30
29
30
31
33
1
Non-Retail
Clinics
76
82
91
101
106
110
45
Non-Federal Hospital
39
39
40
41
39
41
4
Long-Term Care
19
19
19
17
16
16
-17
Home Health Care
4.4
4.8
6.3
7.5
8.2
8.6
95
Federal Facilities
3.0
3.1
3.1
3.2
2.9
2.8
-9
HMO
1.8
2.0
2.1
2.4
2.5
2.1
21
Other
0.6
0.7
0.5
0.6
0.6
0.5
-15
Prisons
0.6
0.6
0.6
0.6
0.5
0.5
-10
Universities
0.32
0.33
0.33
0.32
0.23
0.22
-31
Source: ASPE analysis of IQVIA National Sales Perspective (NSP) Data. All dollar amounts include an adjustment for inflation so they
represent a “real dollar” as of quarter 1 of 2022.
HMO = Health Maintenance Organization
Figure 2 shows the change in the total share of prescriptions filled by location of sale between 2016 and 2021. In
2016, the plurality of retail prescriptions, 43 percent, were purchased at a chain store pharmacy, but by 2021,
there were equal shares of retail drug expenditures at chain store pharmacies and mail order pharmacies (40
percent each). In the non-retail setting, clinics were the most common location of sale in 2016 and they
increased their share of non-retail drug expenditures by 8 percent in 2021. The increase was the result of a 4
percent decrease each in the share of non-retail drug expenditures in non-federal hospitals and long-term care
facilities.

SEPTEMBER 2022 Issue Brief 5
Figure 2. Percent of Spending on each Location of Sale, 2016-2021
Note: Four categories (Health Maintenance Organizations, Other, Prisons, and Universities) were not included because they represented
fewer than 2% of prescriptions in 2016 and 2021)
Source: ASPE analysis of IQVIA National Sales Perspective Data
Brand vs. Generic Drug Changes
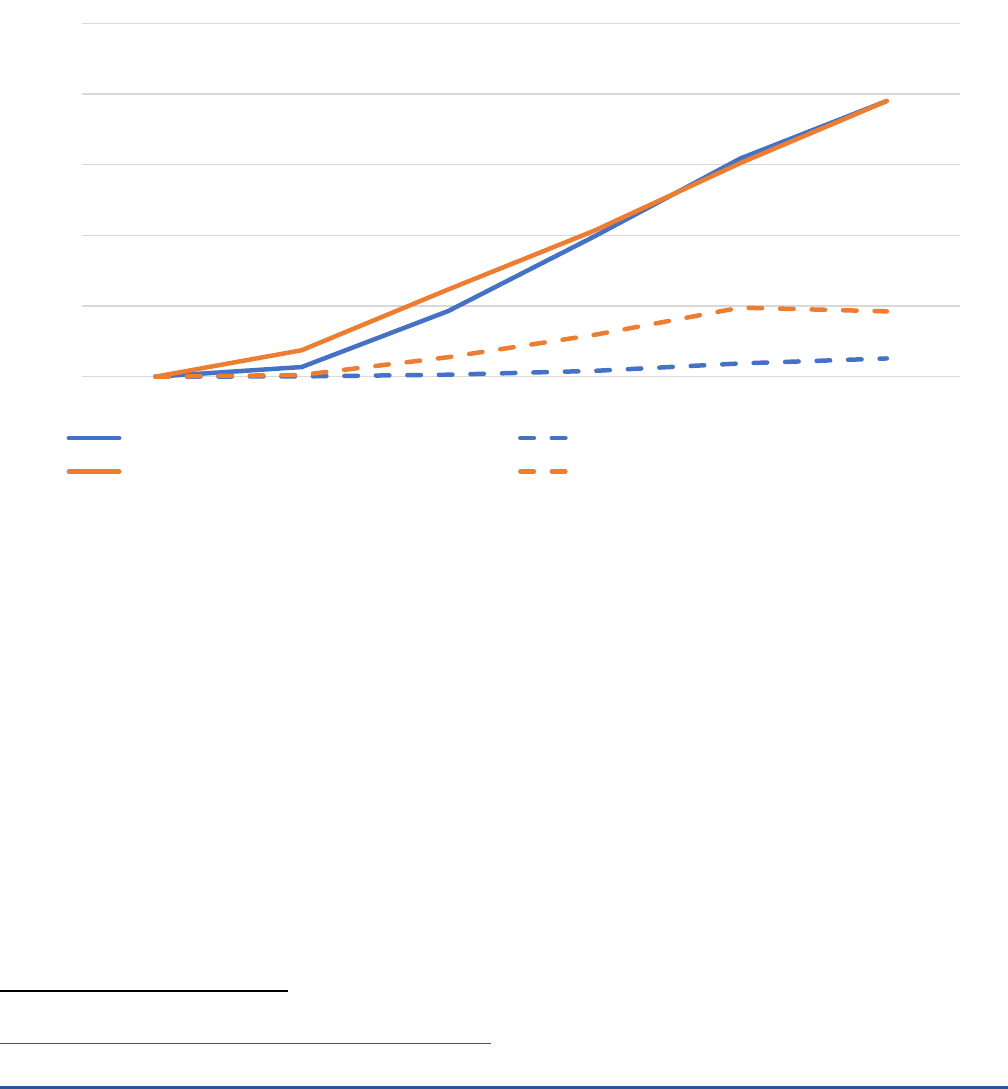
Figure 3 breaks down changes in prescription drug spending and number of prescriptions by brand name versus
generic drugs. Among brand name drugs, there was growth in both retail and non-retail drug expenditures
across the five-year time span, including during 2020. The trend for brand name drug expenditures was
consistent with the trend seen for overall prescription drug spending in Figure 1.
7
The trends in expenditures
and prescriptions for generic drugs were different than for brand name drugs. For generic drugs, from 2016 to
2021, there was a steady decline in retail generic drug expenditures and a steady increase in non-retail generic
drug expenditures.
However, the number of brand name prescriptions varied by year for both brand name and generic drugs.
Among retail brand name prescriptions, there was a growing number of prescriptions from 2016 to 2018 and
then a plateau between 2018 and 2021, with a slight dip in 2020. Despite this variation in the number of
prescriptions, there was a continual increase in total expenditures on brand name drugs throughout this five-
year period, which is likely the result of growth in spending per prescription. For non-retail brand name
prescriptions and retail generic drugs, there was year to year variation, as seen in Figure 3. For non-retail generic
prescriptions, there was some year-to-year fluctuation between 2018 and 2021, but, across the full time period,
there was no change. Examining these trends collectively, utilization increases played a role in increased
expenditures among retail brand name drugs but played no role in expenditure growth for non-retail drugs.
7
For brand name prescription expenditures, the data presented does not include rebates. Rebates for generic drugs and non-retail drugs
are minimal.
43%
33%
16%
9%
52%
27%
13%
3%
40%
40%
13%
8%
60%
23%
9%
5%
0%
10%
20%
30%
40%
50%
60%
70%
Chain Store Pharmacy
Mail Order Pharmacy
Independent Pharmacy
Food Store Pharmacy
Clinics
Non-Federal Hospital
Long-Term Care
Home Health Care
Retail Non-Retail
Series1 Series2
2016 2021

SEPTEMBER 2022 Issue Brief 6
Figure 3. Change in Expenditures (in Inflation Adjusted Dollars) and Prescriptions for Brand Name and Generic
Drugs, 2016-2021
Brand Name Drugs
Generic Drugs
8
Source: ASPE analysis of IQVIA National Sales Perspective Data. All dollar amounts include an adjustment for inflation so
they represent a “real dollar” as of quarter 1 of 2022.
Figure 4 shows the share of all prescriptions and expenditures for brand name drugs from 2016 to 2021. There
was almost no change over this period for either measure. Brand name drugs accounted for 80 percent of
prescription drug expenditures in both retail and non-retail settings, despite accounting for only 20 percent of
retail and non-retail prescriptions, with little change over time. However, there was a noticeable dip in non-
retail prescriptions in 2020 that was likely related to a drop in office visits during the early stages of the COVID-
19 pandemic. However, there was no corresponding dip in spending on non-retail drugs.
8
“Generic drugs” includes both true generics and branded generics
70
80
90
100
110
120
130
140
2016 2017 2018 2019 2020 2021
% As a Share of 2016 Levels
70
80
90
100
110
120
130
140
2016 2017 2018 2019 2020 2021
% as a Share of 2016 Level
Retail Expenditures Retail Prescriptions
Non-Retail Expenditures Non-Retail Prescriptions

SEPTEMBER 2022 Issue Brief 7
Figure 4. Brand Name Drugs as a Share of All Prescription Drug Spending and Prescriptions
9
Source: ASPE analysis of IQVIA National Sales Perspective Data
Specialty Drugs
Table 3 shows trends in specialty drug spending between 2016 and 2021 (see Appendix for definition of
specialty drugs). The overall changes resemble what was evident for all drugs, spending growth was largely due
to higher prices per prescription, not increases in utilization. By 2021, specialty drugs were more than 40
percent of retail drug spending and nearly 70 percent of non-retail drug spending.
10
Specialty drug spending between 2016 and 2021 increased by 43 percent for a total of $301 billion in 2021,
despite there being only a 0.5 percent increase in the number of specialty prescriptions. Disaggregating the data
for the retail and non-retail settings, the percent of retail drug spending on specialty drugs increased 22 percent
between 2016 and 2021. The number of retail prescriptions for specialty drugs increased from 2016 through
2019, but there was a drop in 2020 and 2021. When examining the five-year trend, there was a net 18 percent
drop in the specialty share of retail prescriptions. In contrast, when examining non-retail specialty drugs, the
percent of spending on specialty drugs increased 20 percent over the five-year time horizon and the number of
prescriptions for specialty drugs increased by 40 percent, despite decreases in prescriptions in 2019, 2020, and
2021.
9
The rate of generic drugs as a share of all prescription drug spending and prescriptions is the inverse of the brand name spending and
prescriptions.
10
Rebates for specialty drugs with competition can be substantial, were is not accounted for in this analysis.
10%
20%
30%
40%
50%
60%
70%
80%
90%
2016 2017 2018 2019 2020 2021
Share of Retail Spending Share of Retail Prescriptions
Share of Non-Retail Spending Share of Non-Retail Prescriptions

SEPTEMBER 2022 Issue Brief 8
Table 3. Specialty Drug Expenditures (in Inflation Adjusted Dollars), 2016-2021
Total
Specialty
Spending
Billions, $
Number of
Specialty
Prescriptions
Millions
Retail Spending Non-Retail Spending
% Retail
Spending on
Specialty
% Retail
Prescriptions
on Specialty
% Non-Retail
Spending on
Specialty
% Non-Retail
Prescriptions
on Specialty
2016
211
1,107
34.3
18.9
57.2
6.4
2017
225
1,160
36.5
19.3
60.0
6.8
2018
245
1,443
37.6
21.3
63.6
11.0
2019
268
1,413
39.7
20.4
65.8
9.8
2020
287
1,161
41.3
16.9
67.8
9.1
2021
301
1,113
41.8
15.4
68.8
8.9
% Change
2016-2021
42.5%
0.5%
21.9%
-18.3%
20.3%
40.0%
Source: ASPE analysis of IQVIA data. All dollar amounts include an adjustment for inflation so they represent a “real dollar” as of quarter
1 of 2022.
Figure 5 shows trends over time in the share of retail and non-retail drug spending and prescriptions for
specialty drugs. Between 2016 and 2021, there was a slight increase, up to 10 percent, in the share of both retail
and non-retail spending for specialty drugs. But there was very little change over time in the number of
prescriptions for specialty drugs; the share of retail prescriptions on specialty drugs rarely exceeded 20 percent
and the share of non-retail prescriptions on specialty drugs rarely exceeded 10 percent.
Figure 5. Specialty Drugs as a Share of All Retail Prescription Drug Spending and Prescriptions
Source: ASPE analysis of IQVIA National Sales Perspective Data
0%
10%
20%
30%
40%
50%
60%
70%
80%
2016 2017 2018 2019 2020 2021
Share of Retail Spending Share of Non-Retail Spending
Share of Retail Prescriptions Share of Non-Retail Prescriptions
SEPTEMBER 2022 Issue Brief 9
Over the past decade, there has been a trend towards a larger share of new drug approvals for specialty drugs.
11
Figure 6 shows the annual share of specialty drug spending on new drugs, defined as those drugs introduced
after 2016. By 2021, the share of specialty drug spending on new drugs, in both the retail and non-retail settings,
was 20 percent. Among all specialty drug prescriptions, fewer than 5 percent of prescriptions were for new
drugs, in both the retail and non-retail settings. This means that in the retail setting, 1 percent of prescriptions
for new specialty drugs accounted for 20 percent of spending ($25 billion).
Figure 6. Share of New Drugs (Introduced Since 2016) as a Share of Specialty Drug Spending, 2016-2021
Source: ASPE analysis of IQVIA National Sales Perspective Data
Most Expensive Drugs
Figure 7 shows the share of spending and prescriptions for the top ten percent of drugs by price
12
. The top 10
percent of drugs by price made up 15 percent of retail spending between 2016 and 2021, with little change over
time. The top 10 percent of drugs by price made up 20 to 25 percent of non-retail spending, depending on the
year. For both retail and non-retail prescriptions, the top 10 percent of drugs by price made up less than 1
percent of total prescriptions.
11
Congressional Budget Office. (2021). A Comparison of Brand-Name Drug Prices Among Selected Federal Programs.
https://www.cbo.gov/system/files/2021-02/56978-Drug-Prices.pdf
12
Price was defined as the reported drug price (i.e., gross drug cost before rebates) in the IQVIA data.
0
5
10
15
20
25
2016 2017 2018 2019 2020 2021
Share of Retail Specialty Spending Share of Retail Specialty Prescriptions
Share of Non-Retail Specialty Spending Share of Non-Retail Specialty Prescriptions

SEPTEMBER 2022 Issue Brief 10
Figure 7. Top 10% of Drugs by Price as a Fraction of All Drug Expenditures (in Inflation Adjusted Dollars) on
Prescription Drugs
Source: ASPE analysis of IQVIA National Sales Perspective Data
Conclusion
This brief shows trends in prescription drug spending between 2016 and 2021, disaggregated by retail and non-
retail settings, generic vs. brand drugs, and specialty and high-cost drugs. We found a steady increase in
prescription drug spending from $520 billion in 2016 to $603 billion in 2021. This increase was driven by
increases in spending per prescription, and less so by increases in the number of prescriptions. The largest rate
of growth occurred among non-retail drugs, which increased by 40 percent. There was also a continued increase
in the share of spending on specialty drugs. These trends are a continuation of the findings from an ASPE Issue
Brief that examined prescription drug spending between 2009 and 2015, despite rapid change in the
prescription drug market during this period, including the increase in specialty drugs use and the use of rebates
for high-cost drugs with competition.
13
Despite our time period coinciding with the COVID-19 pandemic, we saw little impact of the pandemic on
prescription drug spending. Among the measures of drug spending we examined, only one measure – brand
name prescriptions – experienced a noticeable change in 2020 and 2021 that was different than the trend
established between 2016 and 2019. This suggests that spending on prescription drugs was not impacted as
significantly by the pandemic as other health care services.
The passage of the Inflation Reduction Act (IRA) of 2022 will introduce several new provisions intended to affect
drug spending trends in the future.
14
The HHS Secretary will have the authority to negotiate drug prices for
13
Observations on Trends in Prescription Drug Spending. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation,
U.S. Department of Health and Human Services. March 2016.
https://aspe.hhs.gov/sites/default/files/migrated_legacy_files//142181/Drugspending.pdf
14
U.S. Congress. (2022). H.R.5376 - Inflation Reduction Act of 2022. https://www.congress.gov/bill/117th-congress/house-bill/5376
0%
5%
10%
15%
20%
25%
30%
2016 2017 2018 2019 2020 2021
Share of Retail Spending Share of Retail Prescriptions
Share of Non-Retail Spending Share of Non-Retail Prescriptions

SEPTEMBER 2022 Issue Brief 11
selected products in Medicare; the first group of drugs for negotiation will be identified in 2023, with negotiated
prices effective starting in 2026.
15
Drugs qualify as negotiation-eligible based on absence of generic or biosimilar
competitors; total spending in Medicare Part B and Medicare Part D; and time elapsed since FDA approval. By
targeting the highest spending drugs without competition, this provision of the IRA aims to slow the rate of
increase in drug spending over time. The IRA also requires manufacturers who raise Medicare Part B and
Medicare Part D drug prices faster than inflation to pay rebates to Medicare. The goal of this policy is to lower
year-over-year increases in the price of prescription drugs, particularly brand name drugs, which make up 80
percent of all prescription drug spending. Since the primary driver of increased prescription drug spending has
been increases in spending per prescription, not greater utilization, discouraging price increases above inflation
for drugs already on the market may help reduce future growth in prescription drug spending. Other IRA
provisions include eliminating Medicare Part D cost-sharing for recommended vaccines and capping Medicare
Part B and Part D insulin cost-sharing at $35 per insulin product per month beginning in 2023; eliminating cost
sharing for beneficiaries in the catastrophic phase of the Part D benefit, expanding the low-income subsidy
program, and ensuring premium stabilization beginning in 2024; and capping beneficiary out-of-pocket
Medicare Part D costs at $2,000 and implementing a new manufacturer discount program beginning in 2025.
These provisions may also impact future drug spending trends.
15
Congressional Research Service. (2022). Selected Health Provisions of the Inflation Reduction Act.
https://crsreports.congress.gov/product/pdf/IF/IF12203
.

SEPTEMBER 2022 Issue Brief 12
Appendix
The variable used to measure the number of prescriptions throughout this brief is the “eaches” variable in IQVIA
data, which is defined as “the number of single items (such as vials, syringes, bottles, or packet of pills)
contained in a unit or shipping package and purchased by pharmacies in a specific time period. An each is not a
single pill or dosage of medicine (unless one package consists of a single dose). An each may be the same as a
unit if the unit does not subdivide into packages.”
Specialty drugs are defined by IQVIA as products used to treat chronic, rare or complex diseases and that meet 4
or more of the following criteria
3
:
• Initiated and maintained by a specialist
• Generally injectable and/or not self-administered
• Products that require an additional level of care in their chain of custody (i.e., refrigerated, frozen,
chemo, biohazard, etc.)
• Expensive (USD $6K annual cost of therapy)
• Unique distribution (e.g., specialty MO, REMS)
• Requires extensive or in-depth monitoring/patient counseling
• Requires reimbursement assistance
• Products that clearly meet the above criteria are defined as Specialty. Products that are borderline (e.g.
meet three, rather than four criteria) will be brought before the Specialty Governance Board for review
and final decision.

SEPTEMBER 2022 Issue Brief 13
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
Office of the Assistant Secretary for Planning and Evaluation
200 Independence Avenue SW, Mailstop 434E
Washington, D.C. 20201
For more ASPE briefs and other publications, visit: aspe.hhs.gov/reports
ABOUT THE AUTHORS
Sonal Parasrampuria is a Social Science Analyst and FDA portfolio lead in the Office of Science and Data Policy in ASPE.
Stephen Murphy is an Economist in the Office of Science and Data Policy in ASPE.
SUGGESTED CITATION
Parasrampuria, S. and Murphy, S. Trends in Prescription Drug Spending, 2016-2021. Washington, DC: Office of the Assistant
Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. September 2022.
COPYRIGHT INFORMATION
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation
as to source, however, is appreciated.
___________________________________
For general questions or general information about ASPE: aspe.hhs.gov/about
