
WORLD
DRUG
REPORT
2018
EXECUTIVE SUMMARY
CONCLUSIONS AND
POLICY IMPLICATIONS
1
9 789211 483048
ISBN 978-92-1-148304-8
© United Nations, June 2018. All rights reserved worldwide.
ISBN: 978-92-1-148304-8
eISBN: 978-92-1-045058-4
United Nations publication, Sales No. E.18.XI.9
This publication may be reproduced in whole or in part and in any form
for educational or non-profit purposes without special permission from
the copyright holder, provided acknowledgement of the source is made.
The United Nations Office on Drugs and Crime (UNODC) would appreciate
receiving a copy of any publication that uses this publication as a source.
Suggested citation:
World Drug Report 2018 (United Nations publication, Sales No. E.18.XI.9).
No use of this publication may be made for resale or any other commercial
purpose whatsoever without prior permission in writing from UNODC.
Applications for such permission, with a statement of purpose and intent of the
reproduction, should be addressed to the Research and Trend Analysis Branch of UNODC.
DISCLAIMER
The content of this publication does not necessarily reflect the views or
policies of UNODC or contributory organizations, nor does it imply any endorsement.
Comments on the report are welcome and can be sent to:
Division for Policy Analysis and Public Affairs
United Nations Office on Drugs and Crime
PO Box 500
1400 Vienna
Austria
Tel: (+43) 1 26060 0
Fax: (+43) 1 26060 5827
E-mail: [email protected]
Website: https://www.unodc.org/wdr2018

1
Drug treatment and health services continue to fall
short: the number of people suffering from drug use
disorders who are receiving treatment has remained
low, just one in six. Some 450,000 people died in
2015 as a result of drug use. Of those deaths,
167,750 were a direct result of drug use disorders,
in most cases involving opioids.
These threats to health and well-being, as well as to
security, safety and sustainable development,
demand an urgent response.
The outcome document of the special session of the
General Assembly on the world drug problem held
in 2016 contains more than 100 recommendations
on promoting evidence-based prevention, care and
other measures to address both supply and demand.
We need to do more to advance this consensus,
increasing support to countries that need it most
and improving international cooperation and law
enforcement capacities to dismantle organized crimi-
nal groups and stop drug trafficking.
The United Nations Office on Drugs and Crime
(UNODC) continues to work closely with its
United Nations partners to assist countries in imple-
menting the recommendations contained in the
outcome document of the special session, in line
with the international drug control conventions,
human rights instruments and the 2030 Agenda for
Sustainable Development.
In close cooperation with the World Health Organi-
zation, we are supporting the implementation of
the International Standards on Drug Use Prevention
and the international standards for the treatment of
drug use disorders, as well as the guidelines on treat-
ment and care for people with drug use disorders in
contact with the criminal justice system.
The World Drug Report 2018 highlights the impor-
tance of gender- and age-sensitive drug policies,
exploring the particular needs and challenges of
women and young people. Moreover, it looks into
Both the range of drugs and drug markets are
expanding and diversifying as never before. The
findings of this year’s World Drug Report make clear
that the international community needs to step up
its responses to cope with these challenges.
We are facing a potential supply-driven expansion
of drug markets, with production of opium and
manufacture of cocaine at the highest levels ever
recorded. Markets for cocaine and methampheta-
mine are extending beyond their usual regions and,
while drug trafficking online using the darknet con-
tinues to represent only a fraction of drug trafficking
as a whole, it continues to grow rapidly, despite
successes in shutting down popular trading
platforms.
Non-medical use of prescription drugs has reached
epidemic proportions in parts of the world. The
opioid crisis in North America is rightly getting
attention, and the international community has
taken action. In March 2018, the Commission on
Narcotic Drugs scheduled six analogues of fentanyl,
including carfentanil, which are contributing to the
deadly toll. This builds on the decision by the
Commission at its sixtieth session, in 2017, to place
two precursor chemicals used in the manufacture
of fentanyl and an analogue under international
control.
However, as this World Drug Report shows, the prob-
lems go far beyond the headlines. We need to raise
the alarm about addiction to tramadol, rates of
which are soaring in parts of Africa. Non-medical
use of this opioid painkiller, which is not under
international control, is also expanding in Asia. The
impact on vulnerable populations is cause for seri-
ous concern, putting pressure on already strained
health-care systems.
At the same time, more new psychoactive substances
are being synthesized and more are available than
ever, with increasing reports of associated harm and
fatalities.
PREFACE
2
WORLD DRUG REPORT 2018
Next year, the Commission on Narcotic Drugs will
host a high-level ministerial segment on the 2019
target date of the 2009 Political Declaration and
Plan of Action on International Cooperation
towards an Integrated and Balanced Strategy to
Counter the World Drug Problem. Preparations are
under way. I urge the international community to
take this opportunity to reinforce cooperation and
agree upon effective solutions.
Yury Fedotov
Executive Director
United Nations Office on Drugs and Crime
increased drug use among older people, a develop-
ment requiring specific treatment and care.
UNODC is also working on the ground to promote
balanced, comprehensive approaches. The Office
has further enhanced its integrated support to
Afghanistan and neighbouring regions to tackle
record levels of opiate production and related secu-
rity risks. We are supporting the Government of
Colombia and the peace process with the Revolu-
tionary Armed Forces of Colombia (FARC) through
alternative development to provide licit livelihoods
free from coca cultivation.
Furthermore, our Office continues to support efforts
to improve the availability of controlled substances
for medical and scientific purposes, while prevent-
ing misuse and diversion – a critical challenge if we
want to help countries in Africa and other regions
come to grips with the tramadol crisis.

3
CONTENTS
PREFACE ...................................................................................................... 1
EXPLANATORY NOTES .................................................................................5
EXECUTIVE SUMMARY ................................................................................7
Latest trends .....................................................................................................................................8
Market developments .....................................................................................................................10
Vulnerabilities of particular groups .................................................................................................15
CONCLUSIONS AND POLICY IMPLICATIONS .............................................. 23
GLOSSARY ................................................................................................. 29
REGIONAL GROUPINGS ............................................................................. 31
BOOKLET 1
EXECUTIVE SUMMARY — CONCLUSIONS AND POLICY IMPLICATIONS
BOOKLET 2
GLOBAL OVERVIEW OF DRUG DEMAND AND SUPPLY
Latest trends, cross-cutting issues
BOOKLET 3
ANALYSIS OF DRUG MARKETS
Opioids, cocaine, cannabis, synthetic drugs
BOOKLET 4
DRUGS AND AGE
Drugs and associated issues among young people and older people
BOOKLET 5
WOMEN AND DRUGS
Drug use, drug supply and their consequences
4
WORLD DRUG REPORT 2018
Acknowledgements
The World Drug Report 2018 was prepared by the Research and Trend Analysis Branch, Division for
Policy Analysis and Public Affairs, United Nations Office on Drugs and Crime, under the supervision
of Jean-Luc Lemahieu, Director of the Division, and Angela Me, Chief of the Research and Trend
Analysis Branch.
General coordination and content overview
Chloé Carpentier
Angela Me
Analysis and drafting
Pablo Carvacho
Conor Crean
Philip Davis
Catalina Droppelmann
Diana Fishbein
Natascha Eichinger
Susan Ifeagwu
Theodore Leggett
Sabrina Levissianos
Kamran Niaz
José Luis Pardo Veiras
Thomas Pietschmann
Fifa Rahman
Martin Raithelhuber
Alejandra Sánchez Inzunza
Claudia Stoicescu
Justice Tettey
Amalia Valdés
Data management and estimates production
Enrico Bisogno
Coen Bussink
Hernan Epstein
Jesus Maria Garcia Calleja (WHO)
Riku Lehtovuori
Tun Nay Soe
Andrea Oterová
Umidjon Rakhmonberdiev
Ali Saadeddin
Keith Sabin (UNAIDS)
Antoine Vella
Editing
Joseph Boyle
Jonathan Gibbons
Graphic design and production
Anja Korenblik
Suzanne Kunnen
Kristina Kuttnig
Coordination
Francesca Massanello
Data support
Diana Camerini
Chung Kai Chan
Sarika Dewan
Smriti Ganapathi
Administrative support
Anja Held
Iulia Lazar
Paul Griffiths
Marya Hynes
Vicknasingam B. Kasinather
Letizia Paoli
Charles Parry
Peter Reuter
Francisco Thoumi
Alison Ritter
In memoriam
Brice de Ruyver
Review and comments
The World Drug Report 2018 benefited from the expertise of and invaluable contributions from
UNODC colleagues in all divisions.
The Research and Trend Analysis Branch acknowledges the invaluable contributions and advice
provided by the World Drug Report Scientific Advisory Committee:
The research and production of the joint UNODC/UNAIDS/WHO/World Bank estimates of
the number of people who inject drugs were partly funded by the HIV/AIDS Section of the Drug
Prevention and Health Branch of the Division for Operations of UNODC.
The research for booklets 4 and 5 was made possible by the generous contribution of Germany
(German Agency for International Cooperation (GIZ)).

5
EXPLANATORY NOTES
The boundaries and names shown and the designa-
tions used on maps do not imply official endorsement
or acceptance by the United Nations. A dotted line
represents approximately the line of control in
Jammu and Kashmir agreed upon by India and Paki-
stan. The final status of Jammu and Kashmir has
not yet been agreed upon by the parties. Disputed
boundaries (China/India) are represented by cross-
hatch owing to the difficulty of showing sufficient
detail.
The designations employed and the presentation of
the material in the World Drug Report do not imply
the expression of any opinion whatsoever on the
part of the Secretariat of the United Nations con-
cerning the legal status of any country, territory, city
or area, or of its authorities or concerning the delimi-
tation of its frontiers or boundaries.
Countries and areas are referred to by the names
that were in official use at the time the relevant data
were collected.
All references to Kosovo in the World Drug Report,
if any, should be understood to be in compliance
with Security Council resolution 1244 (1999).
Since there is some scientific and legal ambiguity
about the distinctions between “drug use”, “drug
misuse” and “drug abuse”, the neutral terms “drug
use” and “drug consumption” are used in the World
Drug Report. The term “misuse” is used only to
denote the non-medical use of prescription drugs.
All uses of the word “drug” in the World Drug Report
refer to substances controlled under the international
drug control conventions.
All analysis contained in the World Drug Report is
based on the official data submitted by Member
States to the United Nations Office on Drugs and
Crime through the annual report questionnaire
unless indicated otherwise.
The data on population used in the World Drug
Report are taken from: World Population Prospects:
The 2017 Revision (United Nations, Department of
Economic and Social Affairs, Population Division).
References to dollars ($) are to United States dollars,
unless otherwise stated.
References to tons are to metric tons, unless other-
wise stated.
The following abbreviations have been used in the
present booklet:
GHB gamma-Hydroxybutyric acid
ha hectares
LSD Lysergic acid diethylamide
MDMA 3,4-Methylenedioxymethamphetamine
NPS new psychoactive substances
PWID people who inject drugs
UNODC
United Nations Office on Drugs
and Crime
WHO World Health Organization

7
Opioids continued to cause the most harm, account-
ing for 76 per cent of deaths where drug use disorders
were implicated. PWID — some 10.6 million world-
wide in 2016 — endure the greatest health risks. More
than half of them live with hepatitis C, and one in
eight live with HIV.
The headline figures for drug users have changed
little in recent years, but this stability masks the
striking ongoing changes in drug markets. Drugs
such as heroin and cocaine that have been available
for a long time increasingly coexist with NPS and
there has been an increase in the non-medical use
of prescription drugs (either diverted from licit chan-
nels or illicitly manufactured).The use of substances
of unclear origin supplied through illicit channels
that are sold as purported medicines but are destined
for non-medical use is also on the increase. The
range of substances and combinations available to
users has never been wider.
About 275 million people worldwide, which is
roughly 5.6 per cent of the global population aged
15–64 years, used drugs at least once during 2016.
Some 31 million of people who use drugs suffer from
drug use disorders, meaning that their drug use is
harmful to the point where they may need treatment.
Initial estimations suggest that, globally, 13.8 million
young people aged 15–16 years used cannabis in the
past year, equivalent to a rate of 5.6 per cent.
Roughly 450,000 people died as a result of drug use
in 2015, according to WHO. Of those deaths,
167,750 were directly associated with drug use dis-
orders (mainly overdoses). The rest were indirectly
attributable to drug use and included deaths related
to HIV and hepatitis C acquired through unsafe
injecting practices.
EXECUTIVE SUMMARY
cannabis opioids
opiates
Number of past-year users in 2016
cocaine
amphetamines and
prescription stimulants
“ecstasy”
192
million
34
million
34
million
21
million
18
million
19
million

8
WORLD DRUG REPORT 2018
seized globally reached a record high of 91 tons in
2016. Most opiates were seized near the manufac-
turing hubs in Afghanistan.
A notable increase has been seen in cocaine
production
Global cocaine manufacture in 2016 reached its
highest level ever: an estimated 1,410 tons. After
falling during the period 2005–2013, global cocaine
manufacture rose by 56 per cent during the period
2013–2016. The increase from 2015 to 2016 was
25 per cent.
LATEST TRENDS
Record levels of plant-based drug
production have been reached
Afghan opium poppy cultivation drives
record opiate production
Total global opium production jumped by 65 per
cent from 2016 to 2017, to 10,500 tons, easily the
highest estimate recorded by UNODC since it
started monitoring global opium production at the
beginning of the twenty-first century.
A marked increase in opium poppy cultivation and
a gradual increase in opium poppy yields in
Afghanistan resulted in opium production in the
country reaching 9,000 tons in 2017, an increase
of 87 per cent from the previous year. Among the
drivers of that increase were political instability, lack
of government control and reduced economic
opportunities for rural communities, which may
have left the rural population vulnerable to the
influence of groups involved in the drug trade.
The surge in opium poppy cultivation in Afghani-
stan meant that the total area under opium poppy
cultivation worldwide increased by 37 per cent from
2016 to 2017, to almost 420,000 ha. More than 75
per cent of that area is in Afghanistan.
Overall seizures of opiates rose by almost 50 per
cent from 2015 to 2016. The quantity of heroin
Global coca bush cultivation and cocaine
manufacture, 2006–2016
Sources: UNODC, coca cultivation surveys in Bolivia (Plurina-
tional State of), Colombia and Peru, 2014 and previous years.
Opium poppy cultivation and production of opium, 2006-2017
a
Sources: UNODC, calculations are based on UNODC illicit crop monitoring surveys and the responses to the annual report
questionnaire.
a
Data for 2017 are still preliminary.
0
40,000
80,000
120,000
160,000
200,000
240,000
280,000
320,000
360,000
400,000
440,000
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
10,000
11,000
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
Culvaon (hectares)
Producon (tons)
Total area under culvaon
Producon in Afghanistan
Producon in Myanmar
Producon in the
Lao People's Democrac Republic
Producon in Mexico
Producon in other countries
0
300
600
900
1,200
1,500
0
50,000
100,000
150,000
200,000
250,000
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
Potential manufacture of cocaine in tons
(at 100 per cent purity)
Hectares under coca cultivation
Bolivia (Plurinational State of) (ha)
Peru (ha)
Colo mbia (ha)
Global cocaine manufacture ('new' conversion ratio)

9
1
EXECUTIVE SUMMARY
Asia, which had previously accounted for more than
half of global seizures, reported just 7 per cent of
the global total in 2016.
The rise in seizures of pharmaceutical opioids in
Africa is mostly due to the worldwide popularity of
tramadol, an opioid used to treat moderate and
moderate-to-severe pain that is widely trafficked for
non-medical use in the region. Tramadol is smug-
gled to various markets in West and Central Africa
and North Africa, from where some of it is trafficked
onwards to countries in the Near and Middle East.
Countries in those subregions have reported the
rapid expansion of the non-medical use of tramadol,
in particular among some vulnerable populations.
The drug is not yet under international control and
is perceived by recreational users as a way of boost-
ing energy and improving mood. However, tramadol
can produce physical dependence, with WHO stud-
ies showing that this dependence may occur when
it is used daily for more than a few weeks.
While some tramadol is diverted from licit channels,
most of the tramadol seized worldwide in the period
2012–2016 appears to have originated in clandes-
tine laboratories in Asia.
Non-medical use of pharmaceutical
opioids reaches epidemic proportions in
North America
In 2015 and 2016, for the first time in half a cen-
tury, life expectancy in the United States of America
Most of the world’s cocaine comes from Colombia,
which boosted its manufacture by more than one
third from 2015 to 2016, to some 866 tons. The
total area under coca bush cultivation worldwide in
2016 was 213,000 ha, almost 69 per cent of which
was in Colombia.
The dramatic resurgence of coca bush cultivation
in Colombia — which had almost halved from 2000
to 2013 — came about for a number of reasons
related to market dynamics, the strategies of traf-
ficking organizations and expectations in some
communities of receiving compensation for replac-
ing coca bush cultivation, as well as a reduction in
alternative development interventions and in eradi-
cation. In 2006, more than 213,000 ha were
eradicated. Ten years later, the figure was less than
18,000 ha.
The result has been a perceived decrease in the risk
of coca bush cultivation and a dramatic scaling-up
of manufacture. Colombia has seen massive rises in
both the number of cocaine laboratories dismantled
and the amount of cocaine seized.
Non-medical use of prescription
drugs is becoming a major threat
around the world
The non-medical use of pharmaceutical opioids is
of increasing concern for both law enforcement
authorities and public health professionals. Differ-
ent pharmaceutical opioids are misused in different
regions. In North America, illicitly sourced fentanyl,
mixed with heroin or other drugs, is driving the
unprecedented number of overdose deaths. In
Europe, the main opioid of concern remains heroin,
but the non-medical use of methadone, buprenor-
phine and fentanyl has also been reported. In
countries in West and North Africa and the Near
and Middle East, the non-medical use of tramadol,
a pharmaceutical opioid that is not under interna-
tional control, is emerging as a substance of
concern.
Non-medical use of and trafficking in
tramadol are becoming the main drug
threat in parts of Africa
The focus for global seizures of pharmaceutical opi-
oids is now firmly on countries in West and Central
Africa and North Africa, which accounted for 87
per cent of the global total in 2016. Countries in
n
o
n
-
m
e
d
i
c
a
l
u
s
e
o
f
p
r
e
s
c
r
i
p
t
i
o
n
d
r
u
g
s
N
o
r
t
h
A
m
e
r
i
c
a
A
f
r
i
c
a
a
n
d
N
e
a
r
a
n
d
M
i
d
d
l
e
E
a
s
t
tramadol
fentanyl and
its analogues
Fast emerging public health
threats
6
0
c
o
u
n
t
r
i
e
s
benzodiazepines
10
WORLD DRUG REPORT 2018
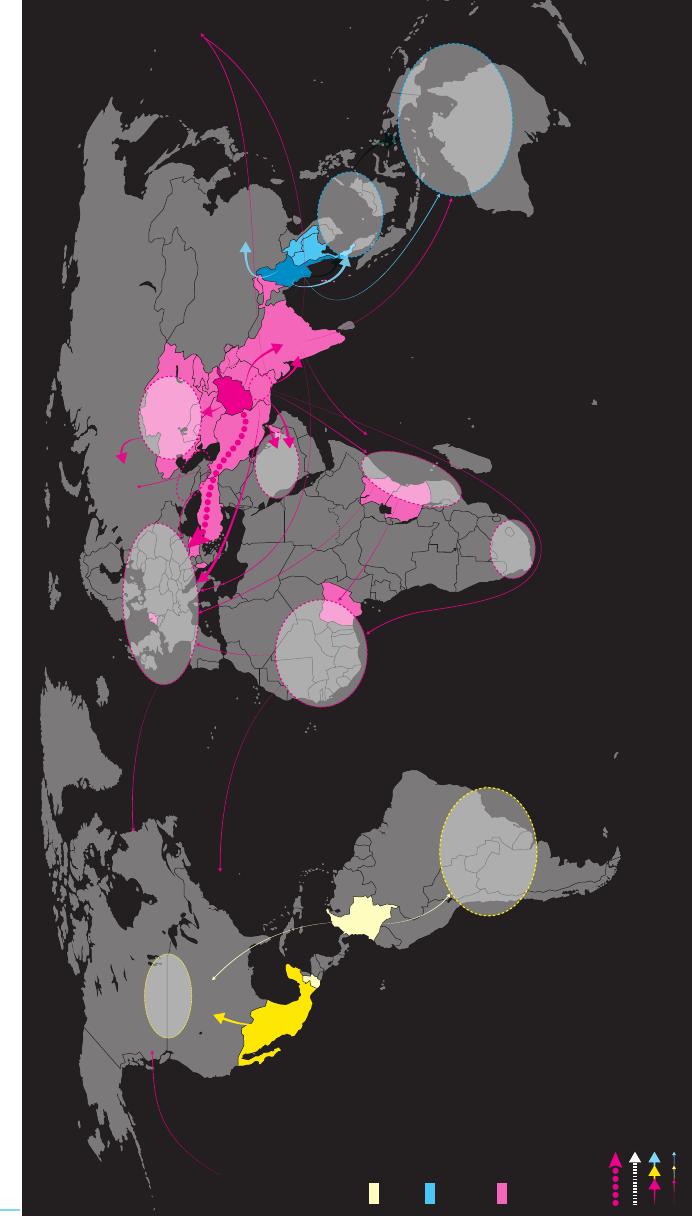
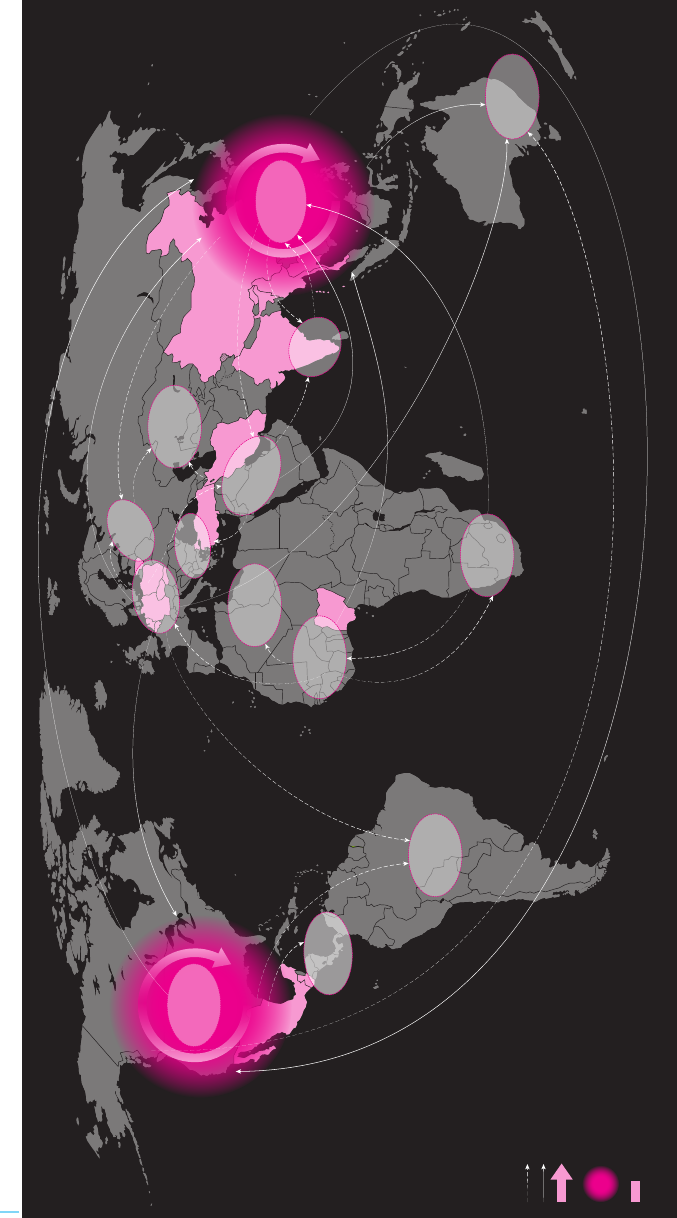
Main heroin trafficking flows, 2012–2016
Sources: UNODC, responses to the annual report questionnaire and individual drug seizure database.
Notes: The size of the trafficking flow lines is based on the amount of heroin seized in a subregion and the number of mentions of countries from where the heroin has departed (including reports of
"origin" and "transit") to a specific subregion over the period 2012–2016. A darker shade indicates that the country represents more than 50 per cent of heroin production in the region. The trafficking
flows are determined on the basis of country of origin/departure, transit and destination of seized drugs as reported by Member States in the annual report questionnaire and individual drug seizure
database: as such, they need to be considered as broadly indicative of existing trafficking routes while several secondary flows may not be reflected. Flow arrows represent the direction of trafficking:
origins of the arrows indicate either the area of manufacture or the one of last provenance, end points of arrows indicate either the area of consumption or the one of next destination of trafficking.
The boundaries shown on this map do not imply official endorsement or acceptance by the United Nations. Dashed lines represent undetermined boundaries. The dotted line represents approximately
the Line of Control in Jammu and Kashmir agreed upon by India and Pakistan. The final status of Jammu and Kashmir has not yet been agreed upon by the parties. The final boundary between the
Republic of Sudan and the Republic of South Sudan has not yet been determined. A dispute exists between the Governments of Argentina and the United Kingdom of Great Britain and Northern
Ireland concerning sovereignty over the Falkland Islands (Malvinas).
Lorem ipsum
Sources: UNODC, responses to annual report questionnaire and individual drug seizure database.
Notes: The size of the trafficking flow lines is based on the amount of heroin seized in a subregion and the number of mentions of countries from where the heroin has departed (including reports of ‘origin’ and transit”) to a specific subregion over the 2012-2016 period. A darker shade indicates that the
country represents more than 50 percent of heroin production in the region. The trafficking flows are determined on the basis of country of origin/departure, transit and destination of seized drugs as reported by Member States in the annual report questionnaire and individual drug seizure database: as
such, they need to be considered as broadly indicative of existing trafficking routes while several secondary flows may not be reflected. Flow arrows represent the direction of trafficking: origins of the arrows indicate either the area of manufacture or the one of last provenance, end points of arrows indicate
either the area of consumption or the one of next destination of trafficking.
The boundaries shown on this map do not imply official endorsement or acceptance by the United Nations. Dashed lines represent undetermined boundaries. The dotted line represents approximately the Line of Control in Jammu and Kashmir agreed upon by India and Pakistan. The final status of Jammu
and Kashmir has not yet been agreed upon by the parties. The final boundary between the Republic of Sudan and the Republic of South Sudan has not yet been determined. A dispute exists between the Governments of Argentina and the United Kingdom of Great Britain and Northern Ireland concerning
sovereignty over the Falkland Islands (Malvinas).
Most frequently mentioned
provenance/transit countries of seized
opiates produced in Latin America
Most frequently mentioned
provenance/transit countries of seized
opiates produced in Myanmar/Lao
People’s Democratic Republic
Most frequently mentioned
provenance/transit countries of seized
opiates produced in Afghanistan
Global heroin trafficking flows by size of
flows estimated on the basis of reported
seizures, 2012-2016:
CENTRAL
ASIA
SOUTH-EAST
ASIA
WESTERN, CENTRAL AND
SOUTH EASTERN EUROPE
GULF AREA
&
MIDDLE EAST
SOUTH
AMERICA
WEST
AFRICA
EAST
AFRICA
OCEANIA
SOUTHERN
AFRICA
Sources: UNODC, responses to annual report questionnaire and individual drug seizure database.
Notes: The size of the trafficking flow lines is based on the amount of heroin seized in a subregion and the number of mentions of countries from where the heroin has departed (including reports of ‘origin’ and transit”) to a specific subregion over the 2012-2016 period. A darker shade indicates that the
country represents more than 50 percent of heroin production in the region. The trafficking flows are determined on the basis of country of origin/departure, transit and destination of seized drugs as reported by Member States in the annual report questionnaire and individual drug seizure database: as
such, they need to be considered as broadly indicative of existing trafficking routes while several secondary flows may not be reflected. Flow arrows represent the direction of trafficking: origins of the arrows indicate either the area of manufacture or the one of last provenance, end points of arrows indicate
either the area of consumption or the one of next destination of trafficking.
The boundaries shown on this map do not imply official endorsement or acceptance by the United Nations. Dashed lines represent undetermined boundaries. The dotted line represents approximately the Line of Control in Jammu and Kashmir agreed upon by India and Pakistan. The final status of Jammu
and Kashmir has not yet been agreed upon by the parties. The final boundary between the Republic of Sudan and the Republic of South Sudan has not yet been determined. A dispute exists between the Governments of Argentina and the United Kingdom of Great Britain and Northern Ireland concerning
sovereignty over the Falkland Islands (Malvinas).
Most frequently mentioned
provenance/transit countries of seized
opiates produced in Latin America
Most frequently mentioned
provenance/transit countries of seized
opiates produced in Myanmar/Lao
People’s Democratic Republic
Most frequently mentioned
provenance/transit countries of seized
opiates produced in Afghanistan
PAKISTAN
AFGHANISTAN
ISLAMIC
REPUBLIC
OF IRAN
TURKEY
MYANMAR
CHINA
RUSSIAN
FEDERATION
MEXICO
PAKISTAN,
INDIA
COLOMBIA
UNITED STATES
OF AMERICA
CANADA
CANADA
LAO PDR
INDIA
CAUCASUS
TANZANIA
(UNITED
REPUBLIC OF)
GUATEMALA
NIGERIA
KENYA
NETHERLANDS
THAILAND
KAZAKHSTAN
UZBEKISTAN
TURKMENISTAN
KYRGYZSTAN
TAJIKISTAN
BULGARIA
ALBANIA
NORTH
AMERICA

11
1
EXECUTIVE SUMMARY
A market for non-controlled benzodiazepine-type
substances, used alone or in combination with con-
trolled benzodiazepines, is emerging in some
Western countries. These substances are marketed
legally as tranquillizers and are sold under names
such as “legal benzodiazepines” or “designer benzo-
diazepines”. In specific cases, a large proportion of
drug-related deaths is related to benzodiazepine-type
NPS.
Kratom, a plant-based substance
used as traditional medicine in some
parts of Asia, is emerging as a popular
plant-based new psychoactive
substance
Kratom products are derived from the leaf of the
kratom tree, which is used in South-East Asia as a
traditional remedy for minor ailments and for non-
medical purposes. Few countries have placed kratom
under national legal control, making it relatively
easy to buy.
There are now numerous products around the world
advertised as containing kratom, which usually come
mixed with other substances. People who use opi-
oids in the United States have reported using kratom
products for the self-management of withdrawal
symptoms. Some 500 tons of kratom were inter-
cepted during 2016, triple the amount of the
previous year, suggesting a boom in its popularity.
MARKET DEVELOPMENTS
Cannabis remains the world’s most
commonly used drug
Cannabis was the most commonly used drug in 2016,
with 192 million people using it at least once in the
past year. The global number of cannabis users con-
tinues to rise and appears to have increased by roughly
16 per cent in the decade ending 2016, which is in
line with the increase in the world population.
The quantities of cannabis herb seized globally
declined by 27 per cent, to 4,386 tons, in 2016. The
decline was particularly marked in North America,
where the availability of medical cannabis in many
jusrisdictions and the legalization of cannabis for rec-
reational use in several states of the United States may
have played a role.
declined for two consecutive years. A key factor was
the increase in unintentional injuries, which includes
overdose deaths.
In 2016, 63,632 people died from a drug overdose
in the United States, the highest number on record
and a 21 per cent increase from the previous year.
This was largely due to a rise in deaths associated
with pharmaceutical opioids, including fentanyl and
fentanyl analogues. This group of opioids, exclud-
ing methadone, was implicated in 19,413 deaths in
the country, more than double the number in 2015.
Evidence suggests that Canada is also affected, with
a large number of overdose deaths involving fentanyl
and its analogues in 2016.
Illicit fentanyl and its analogues are reportedly mixed
into heroin and other drugs, such as cocaine and
MDMA, or “ecstasy”, or sold as counterfeit prescrip-
tion opioids. Users are often unaware of the contents
of the substance they are taking, which inevitably
leads to a great number of fatal overdoses.
Outside North America, the impact of fentanyl and
its analogues is relatively low. In Europe, for exam-
ple, opiates such as heroin and morphine continue
to predominate, although some deaths involving
fentanyl analogues have started to emerge in the
region. A notable exception is Estonia, where fen-
tanyl has long been regarded as the most frequently
misused opioid. The downward trend in opiate use
since the late 1990s observed in Western and Cen-
tral Europe appears to have come to an end in 2013.
In that subregion as a whole, 12 countries reported
stable trends in heroin use in 2016, two reported a
decline and three an increase.
Misuse of sedatives and stimulants brings
growing risks
Many countries are now reporting the
non-medical use of benzodiazepines as
one of the main drug use problems
Non-medical use of the common sedative/hypnotic
benzodiazepines and similar substances is now one
of the main drug use problems in some 60
countries.
The misuse of benzodiazepines carries serious risks,
not least an increased risk of overdose when used in
combination with heroin. Benzodiazepines are fre-
quently reported in fatal overdose cases involving
opioids such as methadone.

12
WORLD DRUG REPORT 2018
Main cocaine trafficking flows, 2012–2016
Sources: UNODC, responses to the annual report questionnaire and individual drug seizure database.
Notes: The size of the trafficking flow lines is based on the amount of cocaine seized in a subregion and the number of mentions of countries from where the cocaine has departed (including reports of
"origin" and "transit") to a specific subregion over the period 2012–2016. The trafficking flows are determined on the basis of country of origin/departure, transit and destination of seized drugs as
reported by Member States in the annual report questionnaire and individual drug seizure database: as such, they need to be considered as broadly indicative of existing trafficking routes while several
secondary flows may not be reflected. Flow arrows represent the direction of trafficking: origins of the arrows indicate either the area of manufacture or the one of last provenance, end points of
arrows indicate either the area of consumption or the one of next destination of trafficking.
The boundaries shown on this map do not imply official endorsement or acceptance by the United Nations. Dashed lines represent undetermined boundaries. The dotted line represents approximately
the Line of Control in Jammu and Kashmir agreed upon by India and Pakistan. The final status of Jammu and Kashmir has not yet been agreed upon by the parties. The final boundary between the
Republic of Sudan and the Republic of South Sudan has not yet been determined. A dispute exists between the Governments of Argentina and the United Kingdom of Great Britain and Northern
Ireland concerning sovereignty over the Falkland Islands (Malvinas).
Most frequently mentioned countries
of provenance as reported by countries
where cocaine seizures took place
Sources: UNODC, responses to annual report questionnaire and individual drug seizure database.
Notes: The size of the trafficking flow lines is based on the amount of cocaine seized in a subregion and the number of mentions of countries from where the cocaine has departed (including reports of ‘origin’ and transit”) to a specific subregion over the 2012-2016 period. The trafficking flows are determined on the basis
of country of origin/departure, transit and destination of seized drugs as reported by Member States in the annual report questionnaire and individual drug seizure database: as such, they need to be considered as broadly indicative of existing trafficking routes while several secondary flows may not be reflected. Flow arrows
represent the direction of trafficking: origins of the arrows indicate either the area of manufacture or the one of last provenance, end points of arrows indicate either the area of consumption or the one of next destination of trafficking.
The boundaries shown on this map do not imply official endorsement or acceptance by the United Nations. Dashed lines represent undetermined boundaries. The dotted line represents approximately the Line of Control in Jammu and Kashmir agreed upon by India and Pakistan. The final status of Jammu and Kashmir has
not yet been agreed upon by the parties. The final boundary between the Republic of Sudan and the Republic of South Sudan has not yet been determined. A dispute exists between the Governments of Argentina and the United Kingdom of Great Britain and Northern Ireland concerning sovereignty over the Falkland Islands
(Malvinas).
Global cocaine trafficking flows by size of
flows estimated on the basis of reported
seizures, 2012-2016:
NORTH
AMERICA
SOUTH
AMERICA
WESTERN
AND CENTRAL
EUROPE
WEST
AFRICA
CENTRAL
AMERICA
CARIBBEAN
SOUTH-EAST
ASIA
SOUTH
ASIA
NEAR AND
MIDDLE EAST
SOUTHERN
AFRICA
EAST AND
SOUTH-EAST
ASIA
OCEANIA
SOUTH-EAST ASIA,
OCEANIA
OCEANIA
SOUTH-EAST
EUROPE
ANDEAN
COUNTRIES
SOUTH
AFRICA
MEXICO
BOLIVIA
(PLUR STATE OF)
BRAZIL
PERU
COLOMBIA
VENEZUELA
(BOL. REP. OF)
CHILE
PARAGUAY
SPAIN
ECUADOR
PORTUGAL
ARGENTINA
NIGERIA
NETHERLANDS
UNITED
ARAB
EMIRATES
PANAMA
GUATEMALA
DOMINICAN REPUBLIC
TRINIDAD AND
TOBAGO
BELGIUM
HONDURAS
French Guiana
(FRANCE)

13
1
EXECUTIVE SUMMARY
for non-medical use through pharmacies began, as
did the sale of the drug through a network of 16
pharmacies.
Effect of the crackdown on darknet
drug dealers is not yet clear
In July 2017, police forces from several countries
worked together to take down the largest drug-trad-
ing platform on the darknet, the part of the “deep
web” containing information that is only accessible
using special web browsers. Before it was closed,
AlphaBay had featured more than 250,000 listings
for illegal drugs and chemicals. It had had over
200,000 users and 40,000 vendors during its exist-
ence. The authorities also succeeded in taking down
the trading platform Hansa, described as the third
largest criminal marketplace on the dark web.
It is not yet clear what effect the closures will have.
According to an online survey in January 2018, 15
per cent of those who had used darknet sites for
purchasing drugs said that they had used such mar-
kets less frequently since the closures, and 9 per cent
said they had completely stopped. However, more
than half did not consider themselves to have been
affected by the closures.
Although the scale of drug trafficking on the dark-
net remains limited, it has shown signs of rapid
growth. Authorities in Europe estimated that drug
sales on the darknet from 22 November 2011 to 16
February 2015 amounted to roughly $44 million
per year. However, a later study estimated that, in
early 2016, drug sales on the darknet were between
$14 million and $25 million per month, equivalent
to between $170 million and $300 million per year.
Africa and Asia have emerged as
cocaine trafficking and consumption
hubs
Most indicators from North America suggest that
cocaine use rose between 2013 and 2016. In 2013,
there were fewer than 5,000 cocaine-related deaths
in the United States, but by 2016 the figure was
more than 10,000. Although many of those deaths
also involved synthetic opioids and cannot be attrib-
uted exclusively to higher levels of cocaine
consumption, the increase is nonetheless a strong
indicator of increasing levels of harmful cocaine use.
Too early to determine the impact
of latest developments in recreational
cannabis regulations
Since 2017, the non-medical use of cannabis has
been allowed in eight state-level jurisdictions in the
United States, in addition to the District of Colum-
bia. Colorado was one of the first states to adopt
measures to allow the non-medical use of cannabis
in the United States. Cannabis use has increased
significantly among the population aged 18–25 years
and older in Colorado since legalization, while it
has remained relatively stable among those aged
17–18 years. However, there has been a significant
increase in cannabis-related emergency room visits,
hospital admissions and traffic deaths, as well as
instances of people driving under the influence of
cannabis in the State of Colorado.
In Uruguay, up to 480 grams per person per year of
cannabis can now be obtained through pharmacies,
cannabis clubs or individual cultivation. Cannabis
regulation in the country allows for the availability
of cannabis products with a tetrahydrocannabinol
content of up to 9 per cent and a minimum can-
nabidiol content of 3 per cent. In mid-2017, the
registration of those who choose to obtain cannabis
1,129
tons
158
tons
70
tons
22
tons
87
tons
156
tons
658
tons
6,313
tons
14
tons
opium
heroin and morphine pharmaceutical opioids
cocainecannabis (herb/resin)
“ecstasy”amphetamine
methamphetamine
synthetic NPS
Quantities of drugs
seized in 2016
14
WORLD DRUG REPORT 2018
Main methamphetamine trafficking flows, 2012–2016
Sources: UNODC, responses to the annual report questionnaire and individual drug seizure database.
Notes: The size of the trafficking flow lines is based on the amount of methamphetamine seized in a subregion and the number of mentions of countries from where the methamphetamine has
departed (including reports of "origin" and "transit") to a specific subregion over the period 2012–2016. The trafficking flows are determined on the basis of country of origin/departure, transit and
destination of seized drugs as reported by Member States in the annual report questionnaire and individual drug seizure database: as such, they need to be considered as broadly indicative of existing
trafficking routes while several secondary flows may not be reflected. Flow arrows represent the direction of trafficking: origins of the arrows indicate either the area of manufacture or the one of last
provenance, end points of arrows indicate either the area of consumption or the one of next destination of trafficking.
The boundaries shown on this map do not imply official endorsement or acceptance by the United Nations. Dashed lines represent undetermined boundaries. The dotted line represents approximately
the Line of Control in Jammu and Kashmir agreed upon by India and Pakistan. The final status of Jammu and Kashmir has not yet been agreed upon by the parties. The final boundary between the
Republic of Sudan and the Republic of South Sudan has not yet been determined. A dispute exists between the Governments of Argentina and the United Kingdom of Great Britain and Northern Ire-
land concerning sovereignty over the Falkland Islands (Malvinas).
Frequently mentioned countries of provenance as reported
by countries where methamphetamine seizures took place
Principal flows
Main markets
NORTH
AMERICA
EASTERN
EUROPE
SOUTH-EAST
EUROPE
WEST
AFRICA
CENTRAL
AMERICA
SOUTH
ASIA
NEAR AND
MIDDLE EAST
SOUTHERN
AFRICA
EAST AND
SOUTH-EAST
ASIA
AUSTRALIA
AND
NEW ZEALAND
Sources: UNODC, responses to annual report questionnaire and individual drug seizure database.
Notes: The size of the trafficking flow lines is based on the amount of methamphetamine seized in a subregion and the number of mentions of countries from where the methamphetamine has departed (including reports of ‘origin’ and transit”) to a specific subregion over the 2012-2016 period.
The trafficking flows are determined on the basis of country of origin/departure, transit and destination of seized drugs as reported by Member States in the annual report questionnaire and individual drug seizure database: as such, they need to be considered as broadly indicative of existing trafficking routes while several secondary
flows may not be reflected. Flow arrows represent the direction of trafficking: origins of the arrows indicate either the area of manufacture or the one of last provenance, end points of arrows indicate either the area of consumption or the one of next destination of trafficking.
The boundaries shown on this map do not imply official endorsement or acceptance by the United Nations. Dashed lines represent undetermined boundaries. The dotted line represents approximately the Line of Control in Jammu and Kashmir agreed upon by India and Pakistan. The final status of Jammu and Kashmir has not yet
been agreed upon by the parties. The final boundary between the Republic of Sudan and the Republic of South Sudan has not yet been determined. A dispute exists between the Governments of Argentina and the United Kingdom of Great Britain and Northern Ireland concerning sovereignty over the Falkland Islands (Malvinas).
NORTH
AFRICA
CENTRAL ASIA
AND
TRANSCAUCASIA
WESTERN
AND CENTRAL
EUROPE
SOUTH
AMERICA
CARIBBEAN
ISLAMIC
REPUBLIC
OF IRAN
TURKEY
CHINA
MEXICO
NIGERIA
NETHERLANDS
GUATEMALA
BELGIUM
INDIA
THAILAND
MYANMAR
POLAND
GERMANY
CZECHIA
LITHUANIA
Global methamphetamine
trafficking flows by size of
flows estimated on the basis
of reported seizures,
2012-2016:
15
1
EXECUTIVE SUMMARY
market for methamphetamine in East and South-
East Asia and Oceania, where the use of crystalline
methamphetamine in particular has become a key
concern.
For many years, amphetamine dominated synthetic
drug markets in the Near and Middle East and West-
ern and Central Europe, but recent increases in the
quantities seized in North Africa and North America
point to growing activity in other subregions. While
the reasons for the spike in the quantity of ampheta-
mine seized in North Africa are not entirely clear,
it may be related to the trafficking of amphetamine
destined for the large market in the neighbouring
subregion of the Near and Middle East.
Growth in the complexity and diver-
sity of the synthetic drug market is
leading to an increase in related harm
In recent years, hundreds of NPS have been
synthesized and added to the established synthetic
drug market for amphetamine-type substances.
Grouped according to their main pharmacological
effect, the largest portion of NPS reported since
UNODC began monitoring are stimulants, followed
The biggest growth in cocaine seizures in 2016 took
place in Asia and Africa, reflecting the ongoing
spread of cocaine trafficking and consumption to
emerging markets. Although starting from a much
lower level than North America, the quantity of
cocaine seized in Asia tripled from 2015 to 2016;
in South Asia, it increased tenfold. The quantity of
cocaine seized in Africa doubled in 2016, with coun-
tries in North Africa seeing a sixfold increase and
accounting for 69 per cent of all the cocaine seized
in the region in 2016. This was in contrast to previ
-
ous years, when cocaine tended to be seized mainly
in West and Central Africa.
Trafficking in and use of synthetic
drugs expands beyond established
markets, and major markets for
methamphetamine continue to grow
East and South-East Asia and North America remain
the two main subregions for methamphetamine traf-
ficking worldwide. In North America, the availability
of methamphetamine was reported to have increased
between 2013 and 2016, and, in 2016, the drug
was reported to be the second greatest drug threat
in the United States, after heroin.
Based on qualitative assessments, increases in
consumption and manufacturing capacity and
increases in the amounts seized point to a growing
Range of
new psychoactive substances
continues to grow
reported in
2012
reported in
2016
2
6
9
N
P
S
4
7
9
N
P
S
The market
for NPS is in
a constant state
of flux
60 NPS
have disappeared from
the market since 2013
479 different
NPS on the
market in 2016
72 newly
emerging NPS
in 2016

16
WORLD DRUG REPORT 2018
programmes. There was no information on the avail-
ability of antiretroviral therapy for 162 countries.
Drug use and the associated harm are
highest among young people
Surveys on drug use among the general population
show that the extent of drug use among young
people remains higher than that among older people,
although there are some exceptions associated with
the traditional use of drugs such as opium or khat.
Most research suggests that early (12–14 years old)
to late (15–17 years old) adolescence is a critical risk
period for the initiation of substance use and that
substance use may peak among young people aged
18–25 years.
Cannabis is a common drug of choice
for young people
There is evidence from Western countries that the
perceived easy availability of cannabis, coupled with
by cannabinoid receptor agonists and classic
hallucinogens.
A total of 803 NPS were reported in the period
2009–2017. However, while the global NPS market
remains widely diversified, with the exception of a
few substances, NPS do not seem to have established
themselves on drug markets or replaced traditional
drugs on a larger scale.
Although the overall quantity of NPS seized fell in
2016, an increasing number of countries have been
reporting NPS seizures, and concerns have been
growing over the harm caused by the use of NPS.
In several countries, an increasing number of NPS
with opioid effects emerging on the market have
been associated with fatalities. The injecting use of
stimulant NPS also remains a concern, in particular
because of reported associated high-risk injecting
practices. NPS use in prisons and among people on
probation remains an issue of concern in some coun-
tries in Europe, North America and Oceania.
VULNERABILITIES OF
PARTICULAR GROUPS
Many countries still fail to provide
adequate drug treatment and health
services to reduce the harm caused by
drugs
One in six people suffering from drug use disorders
received treatment for those disorders during 2016,
which is a relatively low proportion that has
remained constant in recent years.
Some of the most adverse health consequences of
drug use are experienced by PWID. A global review
of services aimed at reducing adverse health
consequences among PWID has suggested that only
79 countries have implemented both needle and
syringe programmes and opioid substitution therapy.
Only four countries were classified as having high
levels of coverage of both of those types of
interventions.
Information on the availability of HIV testing and
counselling and antiretroviral therapy remains
sparse: only 34 countries could confirm the avail-
ability of HIV-testing programmes for PWID, and
17 countries confirmed that they had no such
Distribution of needle-syringes per PWID per year
>
200
100-200
High coverage
Moderate coverage
<
100
Low coverage
33
needle-syringes
distributed
per PWID globally
High coverage
Moderate coverage
Low coverage
>
40
20-40
<
20
16
OST clients
per 100 PWID
globally
Opioid substitution therapy (OST) clients per 100 PWID
Global targets for the distribution of needle-syringes
and opium substitution therapy missed

17
1
EXECUTIVE SUMMARY
perceptions of a low risk of harm, makes the drug
among the most common substances whose use is
initiated in adolescence. Cannabis is often used in
conjunction with other substances and the use of
other drugs is typically preceded by cannabis use.
Two extreme typologies of drug use
among young people: club drugs in
nightlife settings; and inhalants
among street children
Drug use among young people differs from country
to country and depends on the social and economic
circumstances of those involved.
Two contrasting settings illustrate the wide range of
circumstances that drive drug use among young
people. On the one hand, drugs are used in recrea-
tional settings to add excitement and enhance the
experience; on the other hand, young people living
in extreme conditions use drugs to cope with their
difficult circumstances.
The typologies of drugs used in these two different
settings are quite different. Club drugs such as
“ecstasy”, methamphetamine, cocaine, ketamine,
LSD and GHB are used in high-income countries,
originally in isolated “rave” scenes but later in set-
tings ranging from college bars and house parties to
concerts. The use of such substances is reportedly
much higher among young people. Among young
people living on the street, the most commonly used
drugs are likely to be inhalants, which can include
paint thinner, petrol, paint, correction fluid and
glue.
Many street children are exposed to physical and
sexual abuse, and substance use is part of their
coping mechanism in the harsh environment they
are exposed to on the streets. The substances they
use are frequently selected for their low price, legal
and widespread availability and ability to rapidly
induce a sense of euphoria.
Young people’s path to harmful
substance use is complex
The path from initiation to harmful use of sub-
stances among young people is influenced by factors
that are often out of their control. Factors at the
personal level (including behavioural and mental
health, neurological developments and gene varia-
tions resulting from social influences), the micro
level (parental and family functioning, schools and
peer influences) and the macro level (socioeconomic
and physical environment) can render adolescents
vulnerable to substance use. These factors vary
between individuals and not all young people are
equally vulnerable to substance use. No factor alone
is sufficient to lead to the use of substances and, in
many instances, these influences change over time.
Overall, it is the critical combination of the risk
Substance use
initiation
Positive physical, social
and mental health
Harmful use
of substances
P
r
o
t
e
c
t
i
v
e
f
a
c
t
o
r
s
R
i
s
k
f
a
c
t
o
r
s
• Trauma and childhood
adversity
- child abuse and neglect
• Mental health problems
• Poverty
• Peer substance use and
drug availability
• Negative school climate
• Sensation seeking
Protective factors and risk factors for substance use
• Caregiver involvement
and monitoring
• Health and neurological
development:
- coping skills
- emotional regulation
• Physical safety and
social inclusion
• Safe neighbourhoods
• Quality school environment
Substance
use disorders
18
WORLD DRUG REPORT 2018
Drug use among older people requires
attention
Increases in rates of drug use among older
people are partly explained by ageing
cohorts of drug users
Drug use among the older generation (aged 40 years
and older) has been increasing at a faster rate than
among those who are younger, according to the lim-
ited data available, which are mainly from Western
countries.
People who went through adolescence at a time
when drugs were popular and widely available are
more likely to have tried drugs and, possibly, to have
continued using them, according to a study in the
United States. This pattern fits in particular the so-
called “baby boomer” generation in Western Europe
and North America. Born between 1946 and 1964,
baby boomers had higher rates of substance use
during their youth than previous cohorts; a signifi-
cant proportion continued to use drugs and, now
that they are over 50, this use is reflected in the data.
In Europe, another cohort effect can be gleaned
from data on those seeking treatment for opioid use.
Although the number of opioid users entering treat-
ment is declining, the proportion who were aged
over 40 increased from one in five in 2006 to one
in three in 2013. Overdose deaths reflect a similar
trend: they increased between 2006 and 2013 for
those aged 40 and older but declined for those aged
under 40. The evidence points to a large cohort of
ageing opioid users who started injecting heroin
during the heroin “epidemics” of the 1980s and
1990s.
Older people who use drugs require tai-
lored services, but few treatment pro-
grammes address their specific needs
Older drug users may often have multiple physical
and mental health problems, making effective drug
treatment more challenging, yet little attention has
been paid to drug use disorders among older people.
There were no explicit references to older drug users
in the drug strategies of countries in Europe in 2010
and specialized treatment and care programmes for
older drug users are rare in the region; most initia-
tives are directed towards younger people.
factors that are present and the protective factors
that are absent at a particular stage in a young per-
son’s life that makes the difference in their
susceptibility to drug use. Early mental and behav-
ioural health problems, poverty, lack of opportunities,
isolation, lack of parental involvement and social
support, negative peer influences and poorly
equipped schools are more common among those
who develop problems with substance use than
among those who do not.
Harmful substance use has multiple direct effects
on adolescents. The likelihood of unemployment,
physical health problems, dysfunctional social rela-
tionships, suicidal tendencies, mental illness and
even lower life expectancy is increased by substance
use in adolescence. In the most serious cases, harm-
ful drug use can lead to a cycle in which damaged
socioeconomic standing and ability to develop rela-
tionships feed substance use.
Poverty and a lack of opportunities for
social and economic advancement can
lead young people to become involved in
the drug supply chain
Young people are also known to be involved in the
cultivation, manufacturing and production of and
trafficking in drugs. In the absence of social and
economic opportunities, young people may deal
drugs to earn money or to supplement meagre
wages. Young people affected by poverty or in other
vulnerable groups, such as immigrants, may be
recruited by organized crime groups and coerced
into working in drug cultivation, production, traf-
ficking and local-level dealing. In some
environments, young people become involved in
drug supply networks because they are looking for
excitement and a means to identify with local groups
or gangs. Organized crime groups and gangs may
prefer to recruit children and young adults for drug
trafficking for two reasons: the first is the reckless-
ness associated with younger age groups, even when
faced with the police or rival gangs; the second is
their obedience. Young people involved in the illicit
drug trade in international markets are often part
of large organized crime groups and are used mainly
as “mules”, to smuggle illegal substances across
borders.

19
1
EXECUTIVE SUMMARY
suffer from externalizing behaviour problems such
as conduct disorder, attention-deficit hyperactivity
disorder and anti-social personality disorder. Women
with substance use disorders are reported to have
high rates of post-traumatic stress disorder and may
also have experienced childhood adversity such as
physical neglect, abuse or sexual abuse. Women who
use drugs may also have responsibilities as caregiv-
ers, and their drug use adversely affects their families,
in particular children. Such adverse childhood expe-
riences can be transgenerational and impart the risks
of substance use to the children of women with drug
use disorders.
Post-traumatic stress disorder among women is most
commonly considered to have derived from a his-
tory of repetitive childhood physical and sexual
abuse. Childhood adversity seems to have a different
impact on males and females. Research has shown
that boys who have experienced childhood adversity
use drugs as a means of social defiance. On the other
hand, girls who have experienced adversity are more
likely to internalize it as anxiety, depression and
social withdrawal and are more likely to use sub-
stances for self-medication.
Older drug users account for an increasing
share of deaths directly caused by drug
use
Globally, deaths directly caused by drug use increased
by 60 per cent from 2000 to 2015. People over the
age of 50 accounted for 39 per cent of the deaths
related to drug use disorders in 2015. However, the
proportion of older people reflected in the statistics
has been rising: in 2000, older people accounted for
just 27 per cent of deaths from drug use disorders.
About 75 per cent of deaths from drug use disorders
among those aged 50 and older are linked to the
use of opioids. The use of cocaine and the use of
amphetamines each account for about 6 per cent;
the use of other drugs makes up the remaining 13
per cent.
Women’s drug use differs greatly from
men’s
Non-medical use of tranquillizers and
opioids is common
The prevalence of the non-medical use of opioids
and tranquillizers by women remains at a compa-
rable level to that of men, if not actually higher. On
the other hand, men are far more likely than women
to use cannabis, cocaine and opiates. Women con-
tinue to account for only one in five people in
treatment. The proportion of females in treatment
tends to be higher for tranquillizers and sedatives
than for other substances.
While women who use drugs typically begin using
substances later than men, once they have initiated
substance use, women tend to increase their rate of
consumption of alcohol, cannabis, cocaine and opi-
oids more rapidly than men. This has been
consistently reported among women who use those
substances and is known as “telescoping”. Another
difference is that women are more likely to associate
their drug use with an intimate partner, while men
are more likely to use drugs with male friends.
Women who have experienced childhood
adversity internalize behaviours and may
use drugs to self-medicate
Internalizing problems such as depression and anxi-
ety are much more common among women than
among men. Men are more likely than women to
d
r
u
g
u
s
e
r
s
drug use
disorders
More men than women initiate drug use
but after initiation women move faster
than men towards drug use disorders
d
r
u
g
u
s
e
r
s
“telescoping”

20
WORLD DRUG REPORT 2018
that some drug trafficking organizations may be
more likely to use women as “mules”.
Another narrative has emerged critiquing this
approach and arguing that women might be empow-
ered key actors in the drug world economy. Cases
have also been documented in which women are
key actors in drug trafficking, by choice. Neither
explanation provides a complete picture of women’s
involvement in the drug supply chain — some are
victims, others make their own decisions. Involve-
ment in the illicit drug trade can offer women the
chance to earn money and achieve social mobility,
but it can also exacerbate gender inequalities because
they may still be expected to perform the traditional
gender roles of mothers, housekeepers and wives.
Overall, although a multiplicity of factors are behind
the participation of women in the drug trade, it has
been shown to be shaped by socioeconomic vulner-
ability, violence, intimate relationships and economic
considerations.
Prisoners, in particular women, are at
higher risk for infectious diseases but
are poorly served
People in prisons and other closed settings are at a
much greater risk of contracting infections such as
Women are at a higher risk for infectious
diseases than men
Women make up one third of drug users globally
and account for one fifth of the global estimated
number of PWID.
Women have a greater vulnerabil-
ity than men to HIV, hepatitis C and other
blood-borne infections. Many studies have reported
female gender as an independent predictor of
HIV and/or hepatitis C among PWID, particu-
larly among young women and those who have
recently initiated drug injection.
The relationship between
women and the drug trade is
not well understood
Women may not only be victims
but also active participants in the
drug trade
Women play important roles throughout the drug
supply chain. Criminal convictions of women who
presided over international drug trafficking organi
-
zations — particularly in Latin America, but also
in Africa — attest to this. Women’s involvement in
opium poppy cultivation in Afghanistan and coca
cultivation in Colombia is well documented, as is
the role that women play in trafficking drugs, as
drug mules.
However, there is a lack of consistent data from
Governments to enable a deeper understanding of
those roles: 98 countries provided sex-disaggregated
drug-related crime data to UNODC for the period
2012–2016. Of the people arrested for drug-related
offences in those countries during that period, some
10 per cent were women.
As suggested in several studies, women may become
involved in drug trafficking to sustain their own
drug consumption; however, as shown in other stud-
ies, some women involved in trafficking in drugs
are victims of trafficking in persons, including traf-
ficking for the purposes of sexual exploitation.
Women’s participation in the drug supply chain can
often be attributed to vulnerability and oppression,
where they are forced to act out of fear. Moreover,
women may accept lower pay than men: some
researchers have noted that women may feel com-
pelled to accept lower rates of payment than men
to carry out drug trafficking activities, which means
Women
with drug use
disorders
H
I
V
a
n
d
h
e
p
a
t
i
t
i
s
C
c
h
i
l
d
h
o
o
d
a
d
v
e
r
s
i
t
y
a
n
d
a
b
u
s
e
g
e
n
d
e
r
-
b
a
s
e
d
v
i
o
l
e
n
c
e
p
o
s
t
-
t
r
a
u
m
a
t
i
c
s
t
r
e
s
s
d
i
s
o
r
d
e
r
s
s
t
i
g
m
a
a
n
d
d
i
s
c
r
i
m
i
n
a
t
i
o
n
s
o
c
i
a
l
i
n
e
q
u
a
l
i
t
i
e
s
i
n
c
a
r
c
e
r
a
t
i
o
n
d
y
s
f
u
n
c
t
i
o
n
a
l
f
a
m
i
l
y
Causes and consequences of drug use
disorders among women

21
1
EXECUTIVE SUMMARY
tuberculosis, HIV and hepatitis C than the general
population, but access to treatment and prevention
programmes is often lacking. Even where such pro-
grammes are available, they are not necessarily of
the same standard as those provided in the com-
munity. The lack of access to prevention measures
in many prisons can result in the rapid spread of
HIV and other infections.
People who use heroin are exposed to a severe risk
of death from overdose after release from prison,
especially in the first two weeks. Such deaths are
related to a lowered tolerance to the effects of heroin
use developed after periods of relative abstinence,
including during incarceration. However, released
prisoners are rarely able to access overdose
management interventions, including prevention
medications such as naloxone, or treatment for
substance dependence, including methadone.
Women who are incarcerated have even less access
than their male counterparts to health-care services
to address their drug use, other health conditions
and sexual and reproductive health needs. In addi-
tion, fewer women than men generally receive
enough preparation and support for their return to
their family or to the community in general. Upon
release, women face the combined stigma of their
gender and their status as ex-offenders and face chal
-
lenges, including discrimination, in accessing
health-care and social services.
714,000 female prisoners
9,6 million male prisoners
35% drug offences 19% drug offences
A higher proportion of women than men are in prison
for drug-related offences
Almost 11 million people inject drugs
1.3 million people who inject drugs
are living with HIV
5.5 million are living with hepatitis C
1.0 million are living with both
hepatitis C and HIV
Source: Based on Roy Walmsley, “World prison population list”, 11th ed. (Institute for Criminal Policy Research, 2016)
and Roy Walmsley, “World female imprisonment list”, 4th ed. (Institute for Criminal Policy Research, 2017).
Share of prisoners for drug offences based on 50 Member States (UNODC, Special data collections on persons held in
prisons (2010-2014), United Nations Surveys on Crime Trends and the Operations of Criminal Justice Systems (UN-CTS).

23
CONCLUSIONS AND POLICY IMPLICATIONS
The information presented in the World Drug Report
2018 illustrates the unprecedented magnitude and
complexity of the global drug markets. The adverse
health consequences caused by drug use remain sig-
nificant, drug-related deaths are on the rise and there
are ongoing, concentrated opioid epidemics.
This situation calls for renewed efforts to support
the prevention and treatment of drug use and the
delivery of services aimed at reducing the adverse
health consequences of drug use, in line with targets
3.5 and 3.3 of the Sustainable Development Goals.
Young people need to be made aware not only of
the medical but also of the socioeconomic harm
associated with drug use. Efforts to support the pre-
vention and treatment of drug use also include
providing people who use drugs with the necessary
knowledge and skills to prevent overdoses, includ-
ing through the administration of naloxone;
providing continuity of health-care services for those
in prison and upon their release; and scaling up core
interventions, as outlined in the WHO, UNODC,
UNAIDS Technical Guide for Countries to Set Targets
for Universal Access to HIV Prevention, Treatment and
Care for Injecting Drug Users
, to help prevent the
spread of HIV and hepatitis C among PWID.
These efforts can only be effective if they are based
on scientific evidence and respect for human rights
and if the stigma associated with drug use is removed.
Such stigma can be overcome by increasing under-
standing of drug use disorders as complex,
multifaceted and relapsing chronic conditions that
require continuing care and interventions from
many disciplines.
There are emerging trends that have the potential
to trigger a supply-driven expansion of the illicit
markets for heroin, prescription opioids and cocaine.
These new dynamics are of concern as they can have
a particularly detrimental effect on countries with
limited resources, where they can take a heavy toll
on health and may weaken the security situation.
Tramadol, the double tragedy of
developing countries, requires greater
attention
The rapid expansion in Africa and Asia of the use
of illicitly supplied tramadol, a synthetic opioid used
to treat moderate and moderate-to-severe pain, is
posing serious public health challenges. While many
patients continue to have insufficient access to nec-
essary pain medication and would benefit from
greater accessibility to opioids for medical use, the
increasing flow of synthetic opioids destined for
non-medical consumption could lead to an increase
in the number of people developing opioid use dis-
orders. This puts additional pressure on the already
fragile health systems of the affected countries,
which already struggle to meet basic health-care
needs, in particular those of the poor and disadvan-
taged, and have limited availability and coverage of
services for substance use disorders.
Although the opioid overdose crisis in North Amer
-
ica has received international attention, the growing
problem associated with the non-medical use of
synthetic opioids such as tramadol in developing
countries has remained under-researched and has
so far gone largely unnoticed.
New efforts are needed to better understand the
challenges associated with the illicit supply of syn-
thetic opioids and the problems that their
non-medical use cause to public health in develop-
ing countries. In the spirit of shared responsibility,
the international community has a role in addressing
the challenges faced by affected countries in Asia
and Africa. It needs to invest in improving under-
standing of the nature and cause of the problem and
to help the countries concerned to develop drug
prevention, treatment, care and rehabilitation ser-
vices to minimize the public health problems related
to the non-medical use of prescription opioids such
as tramadol. The flow of synthetic opioids packaged
and destined for non-medical purposes also needs
to be stopped.
24
WORLD DRUG REPORT 2018
Health and security threats posed by
record high production of opiates and the
manufacture of cocaine call for enhanced
coordinated responses by countries
along the supply chain
The massive increase in opiate production in
Afghanistan and cocaine manufacture in Colombia
threatens the security system in those two countries.
In Afghanistan, the increased profits generated by
the record production of opiates are likely to further
fuel instability and insurgency and increase funding
to terrorist groups both inside and outside the coun-
try. The expanding illicit economy, which has made
many communities dependent on the income from
opium poppy cultivation, is also likely to further
constrain the development of the licit economy and
to fuel corruption in Afghanistan. Most of the profit
generated by trafficking in Afghan opiates are made
in the major consumer markets, mainly in Europe
and Asia. Those profits also fund organized crime,
corruption and the illicit economy in destination
countries. The expanding cocaine market in Colom-
bia poses a challenge to the implementation of the
peace accord and it is bound to augment the power
and wealth of trafficking groups in the Americas,
Africa and Europe. The increase in opium poppy
and coca bush cultivation cannot be reversed unless
communities in cultivating areas are provided with
the means to develop an alternative livelihood. In
Colombia, for example, alternative development
initiatives have undergone a period of transition
from an approach based on crop elimination to an
approach based on promoting the rule of law.
The expansion of the global cocaine and opiate mar-
kets suggests that there will be a substantial increase
in the profits derived from drug trafficking and
related illicit financial flows, which may also con-
tribute to the financing of other threats such as
terrorism. The cocaine- and opiate-related economy
is already having a major impact not only on the
licit economy but also on democratic processes. By
threatening the implementation of the rule of law
and governance in general, the illicit drug economy
is having a detrimental impact on the development
of effective, accountable and inclusive institutions
at all levels, undermining efforts to achieve Sustain-
able Development Goal 16. While this phenomenon
was for a long time limited to the main cocaine and
opiate production areas, it is now spreading to tran-
sit countries in Latin America, West Asia and Africa
and has the potential to expand into other regions
such as Central and East Asia, suggesting the pos-
sible extension of that detrimental impact to
destination markets. These dynamics call for more
research to help understand the links between drugs
and terrorism, organized crime and corruption, as
well as coordinated action to invest in long-term
alternative development, integration efforts and
international cooperation.
While the toll on health from cocaine and opiate
consumption has long been borne mainly by coun-
tries that are the destination markets, it is increasingly
becoming a challenge for other regions where
cocaine markets are emerging and opiate markets
seem to be expanding. The increases in opiate pro-
duction and cocaine manufacture will have major
implications for drug use globally. Increasing num-
bers of shipments of opiates from Afghanistan to
destination markets in neighbouring countries and
in Europe, and along the main trafficking routes
worldwide, may have spillover effects in the next
few years. More high-quality, low-cost heroin is
likely to reach consumer markets across the world,
with increased consumption and related harms the
likely consequences. Increased awareness among
users and potential users of the implications of their
behaviour on communities in producing countries
is needed.
The implications of the record cocaine production
in Colombia are already visible in the two main
established markets for the drug, North America
and Western and Central Europe, where there are
signs of an increase in use. It is likely, however, that
some cocaine will also find its way to new markets,
supplying the growing middle class in the large econ-
omies in Asia, where the drug has started to appear,
and with possible spillover along the way, in par-
ticular in Africa.
Timely assessments are needed for countries that
could be affected by increased trafficking to allow
them to understand the magnitude of trafficking
flows and equip themselves appropriately so that
they can provide services to prevent the expansion
of drug use and provide treatment and services in
order to minimize the adverse health consequences

25
1
CONCLUSIONS AND POLICY IMPLICATIONS
that drug use can cause. Comprehensive approaches
need to be implemented that are truly global and
encompass all facets of the current threat.
Health and security threats posed by the
expansion of methamphetamine traffick-
ing also call for enhanced coordinated
responses by countries along the drug
supply chain
In terms of synthetic drugs, the expansion of meth-
amphetamine trafficking in East and South-East
Asia poses a serious health and security challenge to
the population in the subregion. The increasing flow
of methamphetamine is likely to increase the
number of people suffering from the negative health
consequences of methamphetamine use and devel-
oping a substance use disorder, but not all countries
in the subregion are equipped to serve an increasing
demand for treatment. More investment in preven-
tion and treatment and closer collaboration in drug
control will be needed at the regional and interna-
tional level to develop effective responses to these
challenges.
Increasing drug use among older people
requires new responses
There has been an increase in global deaths directly
related to the use of drugs among older people, and
an increase in drug use among older people in the
few countries where information is available. This
calls for targeted efforts to prevent, treat and mini-
mize the impact of drug use among this population
group. There are particular and wide-ranging health
issues that arise from drug use among older users,
in particular for those with a history of drug use
disorders and dependence. Treatment for substance
use is more complicated because there are multiple
physical and mental health issues among older
people who use drugs.
Infrastructure is not yet in place to deal with the
growing number of older drug users and their health
needs over the coming decades. There is often no
explicit reference to older users in drug strategies in
countries with ageing populations, which is where
this issue requires most attention. Specialized treat-
ment and care programmes for older drug users are
rare; most initiatives are directed towards younger
people.
Treatment and care will need to incorporate special-
ized drug treatment programmes with mainstream
health-care and social support services. Novel, inte-
grated and multidisciplinary approaches to care are
required to address the health and social needs of
older drug users.
Effectively addressing and countering the
world drug problem to achieve progress
on sustainable development goals related
to young people and women
The 2030 Agenda for Sustainable Development and
its goals affirm that “there can be no sustainable
development without peace and no peace without
sustainable development”. This draws together the
strands of peace, rule of law, human rights, develop-
ment and equality to form a comprehensive and
forward-looking framework. Countering the world
drug problem and efforts to achieve the Sustainable
Development Goals are thus complementary and
mutually reinforcing.
Goal 4 of the agenda for sustainable development
is aimed at ensuring inclusive and equitable quality
education and to promote lifelong learning oppor-
tunities for all. The entrapment of young people in
both drug use and the illicit drug trade itself poses
distinct barriers in the development of individuals
and communities. Strategies to break the cycle of
vulnerability of young people through science-based
effective prevention, and to provide young people
with the skills, education and opportunities relevant
for legitimate employment, can address that goal.
Goal 5 of the agenda for sustainable development
is aimed at achieving gender equality and empower-
ing all women and girls. To achieve this goal,
strategies to counter the world drug problem need
to consider the special needs of women and the great
level of stigmatization that they endure. Prevention
programmes, treatment interventions for drug use
disorders and alternative development programmes,
as well as the criminal justice response to drug
related offences, need to be gender sensitive.
26
WORLD DRUG REPORT 2018
Preventing drug use and the adverse
health consequence of drug use among
young people requires a culture of
understanding, underpinned by scientific
research
Not all young people are equally vulnerable to sub-
stance use, and once drug use has been initiated,
not all young people are equally vulnerable to the
development of drug use disorders. In many
instances, risk factors associated with drug use dis-
orders are both beyond the control of young people
and preventable.
Preventing the initiation of substance use, as well
as the development of substance use disorders, can
be successful only if protective factors are strength-
ened while risk factors are attenuated or prevented.
The UNODC and WHO International Standards
on Drug Use Prevention contain a summary of the
current scientific evidence on strategies that are
effective in preventing substance use, including drug
use; effective prevention contributing significantly
to the positive engagement of young people with
their families, schools and community. Prevention
interventions need to start at an early age and address
the developmental stage and needs of children, ado-
lescents and young people. For young people who
have initiated substance use, screening and brief
interventions are effective in preventing progression
to substance use disorders.
In some countries, the middle or upper socioeco-
nomic classes are associated with “recreational” use
of drugs, which may be a manifestation of their
purchasing power or reflect their willingness or
opportunity to experiment with drugs. While those
socioeconomic groups may have a greater propensity
to use drugs than lower socioeconomic groups, it is
the lower socioeconomic groups that tend to pay a
higher price for drug use, as they are more likely to
develop drug use disorders. Poverty, along with other
factors such as social exclusion and neighbourhood
deprivation, can have adverse educational, health
and behavioural outcomes and has major implica-
tions for the risk of both initiating drug use and
developing drug use disorders.
Many of the factors influencing substance use
among adolescents, such as mental health conditions
and parental neglect, are also linked with other risk
behaviours and health conditions, such as dropping
out of school, delinquency, aggressiveness, violence
and attempted suicide. Drug use prevention pro-
grammes can help prevent those risk behaviours.
Drug use treatment and HIV prevention,
treatment and care should be tailored to
the specific needs of women
The majority of people who use drugs are men, but
women have specific drug use patterns, as they inter-
nalize traumatic experiences in childhood differently
from men, have different psychiatric comorbidities
and have specific needs when it comes to treatment
and other public health services related to drug use
disorders.
The UNODC and WHO International Standards
for the Treatment of Drug Use Disorders and the
WHO Guidelines for the Identification and Manage-
ment of Substance Use and Substance Use Disorders
in Pregnancy describe how the specific issues and
needs of women in treatment and in the community
can be addressed. These include treatment of medi-
cal and psychiatric comorbidities, responding to
domestic violence and sexual abuse, addressing needs
during pregnancy and sexual and reproductive
health and providing child care, social support and
social care. Treatment programmes can be effective
for women if they are tailored to women’s needs in
all aspects of design and delivery, including location,
staffing, child-friendliness and content. Further-
more, a guide published by UNODC, entitled
Addressing the Specific Needs of Women Who Inject
Drugs: Practical Guide for Service Providers on Gen-
der-Responsive HIV Services, supports efforts to
address the specific needs of women who inject
drugs.
Crime prevention and criminal justice
professionals need to recognize the
distinctive needs and particular back-
grounds of women
When women are brought into contact with the
criminal justice system, it is often for drug-related
offences. In terms of sentencing, a higher propor-
tion of women than men are sentenced for
drug-related offences. As the criminal justice system
is predominantly designed to deal with male offend-
ers, it is often ill equipped to address women’s

27
1
CONCLUSIONS AND POLICY IMPLICATIONS
particular backgrounds (for example, care-providing
responsibilities, history of violence or specific mental
health-care needs) and women may be placed in a
situation of vulnerability and face gender-based ste-
reotypes, stigma and social exclusion. Given the
disproportionate increase in the imprisonment of
women for drug-related offences, sentencing should
be matched with gender-sensitive alternatives to
conviction or punishment in appropriate cases, in
line with the United Nations Rules for the Treat-
ment of Women Prisoners and Non-custodial
Measures for Women Offenders (the Bangkok
Rules). The flexibility inherent in the international
drug control conventions should, to the maximum
extent possible, be used to offer individuals (men,
women and children) with drug use disorders the
possibility to choose treatment as an alternative to
conviction or punishment. The UNODC and
WHO handbook entitled Treatment and Care for
People with Drug Use Disorders in Contact with the
Criminal Justice System contains good practices in
this field.
Women are often more adversely affected by being
incarcerated than men. Prior to going to prison they
may have been subject to physical and sexual abuse
to a greater extent than men and may suffer more
than men from drug use disorders and psychiatric
conditions such as post-traumatic stress disorder.
Women may also suffer the additional psychological
burden of not fulfilling the traditional role of care
providers and, when released, may be subject to
greater stigma than men and lose any social support
that could help them settle in the community.
Women prisoners typically have requirements that
are very different to those of men. As outlined in
the UNODC Handbook on Women and Imprison-
ment, prison management should be gender-sensitive.
The recognition of women’s needs should be
reflected in the management ethos of prisons that
house female inmates, with the management style,
assessment and classification, programmes offered
and health care being adapted accordingly. Consid
-
eration should also be given to the treatment of
female prisoners with children. Prisons should
adhere to the Bangkok Rules.
Providing for the special needs of women in the
criminal justice system for drug-related offences is
not discriminatory but essential.
Crime prevention and criminal justice
professionals also need to recognize the
distinctive needs of children
The international legal framework in the area of
children’s rights, including the Convention on the
Rights of the Child and the United Nations Model
Strategies and Practical Measures on the Elimina-
tion of Violence against Children in the Field of
Crime Prevention and Criminal Justice, are bench-
marks for action targeting children who have
substance use problems or who have committed
drug-related criminal offences and are in contact
with the criminal justice system. The specific vul-
nerabilities and needs of children who come into
contact with the criminal justice system and who
have substance use issues need to be addressed. Vio-
lence against children and the abuse of children
suffering from drug use disorders need to be pre-
vented, while ensuring that treatment and support
is offered to detained children that takes into
account their needs, according to age, sex and other
factors.
More research is needed to help
understand the role of women and
young people in drug supply
Research on the role of women and young people
in the drug supply chain is very scarce. There is a
paucity of research on the involvement of women
and young people in drug cultivation, production
and trafficking. While data and analysis on the drug
supply chain are more widely available at the inter-
national level than those on drug use, the vast
majority of information available is not age- or sex-
disaggregated. There is a need to systematize, across
all data collection and research, a gender- and age-
sensitive approach in order to ensure the availability
of evidence for establishing gender- and age-sensitive
drug policies.
Growing complexity requires research,
investment and innovation
The coexistence on the illicit drug market of estab-
lished drugs, NPS, prescription drugs diverted from
licit channels and a growing stream of substances of
unclear origin that are sold as medicines but are
destined for non-medical use, together with poly-
drug use, polydrug trafficking and the darknet as a
marketplace for drugs, is adding unprecedented
levels of complexity to the drug problem.
28
WORLD DRUG REPORT 2018
Such complexity poses a number of challenges to
the development of appropriate responses. Isolated
actions focusing on single substances or single
responses to the drug problem become ineffective
or counterproductive if the interconnectivity
between drug markets and different types of inter-
ventions are not well understood and taken into
account. In general, most evidence-based prevention
is not substance-specific, as it targets general vulner-
ability factors. In addition, with users consuming a
wide range of substances, some of which may be
new on the market, treatment services need to be
multidimensional and multisectoral. Integrating
programmes for polysubstance use disorders into
public health responses helps to better meet the
needs of users. Forensic and toxicology laboratories
and law enforcement agencies can be successful in
their analysis and actions only if they adopt new
methods and more sophisticated instruments that
can better capture the wide range of psychoactive
substances on the market and the modi operandi
employed by traffickers. With the primary objective
of protecting the health of humankind and maxi
-
mizing access to necessary medications, innovative
strategies and operational interventions are needed
to respond to the continuing emergence of NPS not
yet under control, as well as of new illicitly supplied
medicines for non-medical use.
Most of the current instruments for monitoring
drug issues at the national and international levels
were not designed to capture the new complexity
of the global drug market. Current systems tend to
focus on limited aspects of drug use and supply that
underestimate the magnitude of the interlinkages
between the use of established drugs, the non-med-
ical use of prescription medicines and other
psychoactive substances. Early warning systems can
help to monitor the growing complexity and move
towards a proactive approach. Countries with lim-
ited resources require assistance to collect and
analyse the most basic information. The interna-
tional data-collection system, which uses the
UNODC annual report questionnaire as a basis,
also needs to capture the new reality better in order
to ensure that the international community main-
tains a grasp on the multifaceted drug problem.

29
GLOSSARY
amphetamine-type stimulants — a group of substances
composed of synthetic stimulants controlled under the
Convention on Psychotropic Substances of 1971 and
from the group of substances called amphetamines,
which includes amphetamine, methamphetamine,
methcathinone and the “ecstasy”-group substances
(3,4-methylenedioxymethamphetamine (MDMA) and
its analogues).
amphetamines — a group of amphetamine-type
stimulants that includes amphetamine and
methamphetamine.
annual prevalence — the total number of people of a
given age range who have used a given drug at least
once in the past year, divided by the number of people
of the given age range, and expressed as a percentage.
coca paste (or coca base) — an extract of the leaves of
the coca bush. Purification of coca paste yields cocaine
(base and hydrochloride).
“crack” cocaine — cocaine base obtained from cocaine
hydrochloride through conversion processes to make
it suitable for smoking.
cocaine salt — cocaine hydrochloride.
drug use — use of controlled psychoactive substances
for non-medical and non-scientific purposes, unless
otherwise specified.
new psychoactive substances — substances of abuse,
either in a pure form or a preparation, that are not
controlled under the Single Convention on Narcotic
Drugs of 1961 or the 1971 Convention, but that may
pose a public health threat. In this context, the term
“new” does not necessarily refer to new inventions but
to substances that have recently become available.
opiates — a subset of opioids comprising the various
products derived from the opium poppy plant, includ-
ing opium, morphine and heroin.
opioids — a generic term applied to alkaloids from
opium poppy (opiates), their synthetic analogues
(mainly prescription or pharmaceutical opioids) and
compounds synthesized in the body.
problem drug users — people who engage in the high-
risk consumption of drugs; for example, people who
inject drugs, people who use drugs on a daily basis
and/or people diagnosed with drug use disorders
(harmful use or drug dependence), based on clinical
criteria as contained in the Diagnostic and Statistical
Manual of Mental Disorders (fifth edition) of the
American Psychiatric Association, or the International
Classification of Diseases and Related Health Problems
(tenth revision) of the World Health Organization.
people who suffer from drug use disorders/people with
drug use disorders — a subset of people who use drugs.
People with drug use disorders need treatment, health
and social care and rehabilitation. Harmful use of sub-
stances and dependence are features of drug use
disorders.
harmful use of substances — defined in the International
Statistical Classification of Diseases and Related Health
Problems (tenth revision) as a pattern of use that causes
damage to physical or mental health.
dependence — defined in the International Statistical
Classification of Diseases and Related Health Problems
(tenth revision) as a cluster of physiological, behav-
ioural and cognitive phenomena in which the use of
a substance or a class of substances takes on a much
higher priority for a given individual than other behav-
iours that once had greater value. A central descriptive
characteristic of dependence syndrome is the desire
(often strong, sometimes overpowering) to take psy-
choactive drugs.
substance or drug use disorders — the Diagnostic and
Statistical Manual of Mental Disorders (fifth edition)
of the American Psychiatric Association also refers to
“drug or substance use disorder” as patterns of symp-
toms resulting from the use of a substance despite
experiencing problems as a result of using substances.
Depending on the number of symptoms identified,
substance use disorder may vary from moderate to
severe.
prevention of drug use and treatment of drug use disorders
— the aim of “prevention of drug use” is to prevent
or delay the initiation of drug use, as well as the tran-
sition to drug use disorders. Once a person develops
a drug use disorder, treatment, care and rehabilitation
are needed.

31
REGIONAL GROUPINGS
• East and South-East Asia: Brunei Darussalam,
Cambodia, China, Democratic People’s Republic
of Korea, Indonesia, Japan, Lao People’s
Democratic Republic, Malaysia, Mongolia,
Myanmar, Philippines, Republic of Korea,
Singapore, Thailand, Timor-Leste and Viet Nam
• South-West Asia: Afghanistan, Iran (Islamic
Republic of) and Pakistan
• Near and Middle East: Bahrain, Iraq, Israel,
Jordan, Kuwait, Lebanon, Oman, Qatar, Saudi
Arabia, State of Palestine, Syrian Arab Republic,
United Arab Emirates and Yemen
• South Asia: Bangladesh, Bhutan, India, Maldives,
Nepal and Sri Lanka
• Eastern Europe: Belarus, Republic of Moldova,
Russian Federation and Ukraine
• South-Eastern Europe: Albania, Bosnia and
Herzegovina, Bulgaria, Croatia, Montenegro,
Romania, Serbia, the former Yugoslav Republic of
Macedonia and Turkey
• Western and Central Europe: Andorra, Austria,
Belgium, Cyprus, Czechia, Denmark, Estonia,
Finland, France, Germany, Greece, Hungary,
Iceland, Ireland, Italy, Latvia, Liechtenstein,
Lithuania, Luxembourg, Malta, Monaco,
Netherlands, Norway, Poland, Portugal, San
Marino, Slovakia, Slovenia, Spain, Sweden,
Switzerland and United Kingdom of Great Britain
and Northern Ireland
• Oceania: Australia, Fiji, Kiribati, Marshall Islands,
Micronesia (Federated States of), Nauru, New
Zealand, Palau, Papua New Guinea, Samoa,
Solomon Islands, Tonga, Tuvalu, Vanuatu and
small island territories
The World Drug Report uses a number of regional
and subregional designations. These are not official
designations, and are defined as follows:
• East Africa: Burundi, Comoros, Djibouti, Eritrea,
Ethiopia, Kenya, Madagascar, Mauritius, Rwanda,
Seychelles, Somalia, Uganda and United Republic
of Tanzania
• North Africa: Algeria, Egypt, Libya, Morocco,
South Sudan, Sudan and Tunisia
• Southern Africa: Angola, Botswana, Lesotho,
Malawi, Mozambique, Namibia, South Africa,
Swaziland, Zambia and Zimbabwe
• West and Central Africa: Benin, Burkina Faso,
Cabo Verde, Cameroon, Central African
Republic, Chad, Congo, Côte d’Ivoire,
Democratic Republic of the Congo, Equatorial
Guinea, Gabon, Gambia, Ghana, Guinea,
Guinea-Bissau, Liberia, Mali, Mauritania, Niger,
Nigeria, Sao Tome and Principe, Senegal, Sierra
Leone and Togo
• Caribbean: Antigua and Barbuda, Bahamas,
Barbados, Bermuda, Cuba, Dominica, Dominican
Republic, Grenada, Haiti, Jamaica, Saint Kitts
and Nevis, Saint Lucia, Saint Vincent and the
Grenadines and Trinidad and Tobago
• Central America: Belize, Costa Rica,
El Salvador, Guatemala, Honduras, Nicaragua and
Panama
• North America: Canada, Mexico and United
States of America
• South America: Argentina, Bolivia (Plurinational
State of), Brazil, Chile, Colombia, Ecuador,
Guyana, Paraguay, Peru, Suriname, Uruguay and
Venezuela (Bolivarian Republic of)
• Central Asia and Transcaucasia: Armenia,
Azerbaijan, Georgia, Kazakhstan, Kyrgyzstan,
Tajikistan, Turkmenistan and Uzbekistan

9 789211 483048
ISBN 978-92-1-148304-8
Following last year’s 20
th
anniversary edition, the World Drug Report
2018 is again presented in a special five-booklet format designed
to enhance reader friendliness while maintaining the wealth of
information contained within.
Booklet 1 summarizes the content of the four subsequent substantive
booklets and presents policy implications drawn from their findings.
Booklet 2 provides a global overview of the latest estimates of and
trends in the supply, use and health consequences of drugs. Booklet 3
examines current estimates of and trends in the cultivation, production
and consumption of the three plant-based drugs (cocaine, opiates and
cannabis), reviews the latest developments in cannabis policies and
provides an analysis of the global synthetic drugs market, including
new psychoactive substances. Booklet 4 looks at the extent of drug
use across age groups, particularly among young and older people,
by reviewing the risks and vulnerabilities to drug use in young people,
the health and social consequences they experience and their role in
drug supply, as well as highlighting issues related to the health care
needs of older people who use drugs. Finally, Booklet 5 focuses on
the specific issues related to drug use among women, including the
social and health consequences of drug use and access to treatment
by women with drug use disorders; it also discusses the role played
by women in the drug supply chain.
Like all previous editions, the World Drug Report 2018 is aimed
at improving the understanding of the world drug problem and
contributing towards fostering greater international cooperation for
countering its impact on health and security.
The statistical annex is published on the UNODC website:
https://www.unodc.org/wdr2018
